Why “Chronic Sinusitis” and “Nasal Polyps” Are Misleading Terms
Understanding why modern rhinology is moving beyond these outdated disease labels
For decades, patients and doctors alike have used the term chronic sinusitis to describe persistent inflammation of the sinuses. It is one of the most commonly used diagnoses in ear, nose and throat (ENT) practice.
But there is a problem.
The term chronic sinusitis — or chronic rhinosinusitis (CRS) — is not actually a disease.
It is a description of inflammation, not an explanation of why that inflammation occurs.
In many ways, using the term “chronic sinusitis” today is like respiratory physicians describing asthma, COPD, bronchiectasis, and interstitial lung disease collectively as “chronic lungitis.”
No respiratory specialist would accept such a vague diagnosis. Yet in rhinology, we still routinely use a similarly imprecise term.
As our understanding of sinus disease improves, it is becoming increasingly clear that CRS is not one disease, but a group of very different conditions that share a common symptom — chronic inflammation of the sinus lining.
The Problem With the Term “Chronic Sinusitis”
The word sinusitis simply means inflammation of the sinuses.
But inflammation is a final pathway, not a diagnosis.
Inflammation can be caused by many different mechanisms:
-
allergy
-
immune dysregulation from the epithelial barrier
-
infection
-
genetic disease
-
mucociliary dysfunction
Grouping all of these under the same label risks oversimplifying the disease and potentially misdirecting treatment.
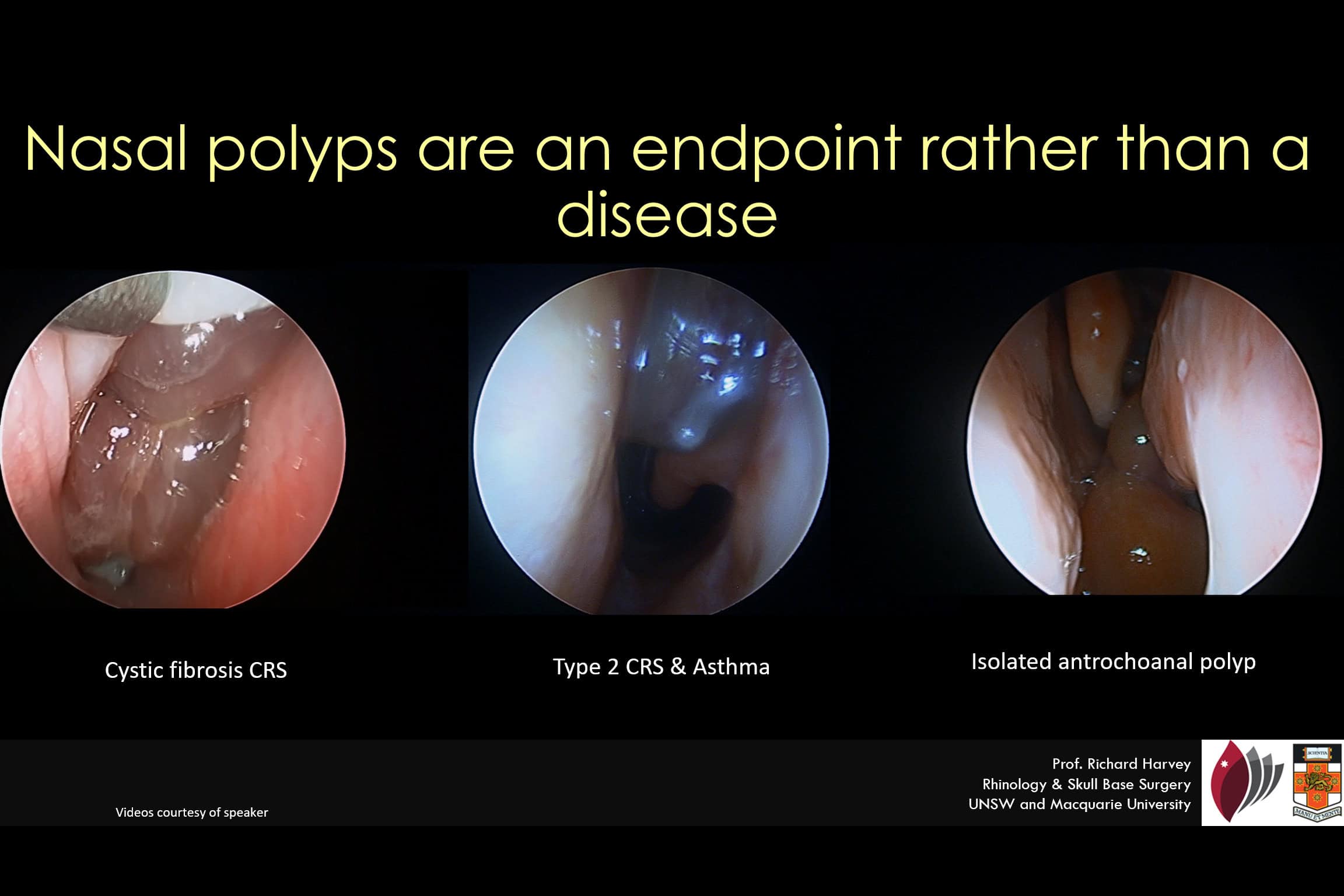
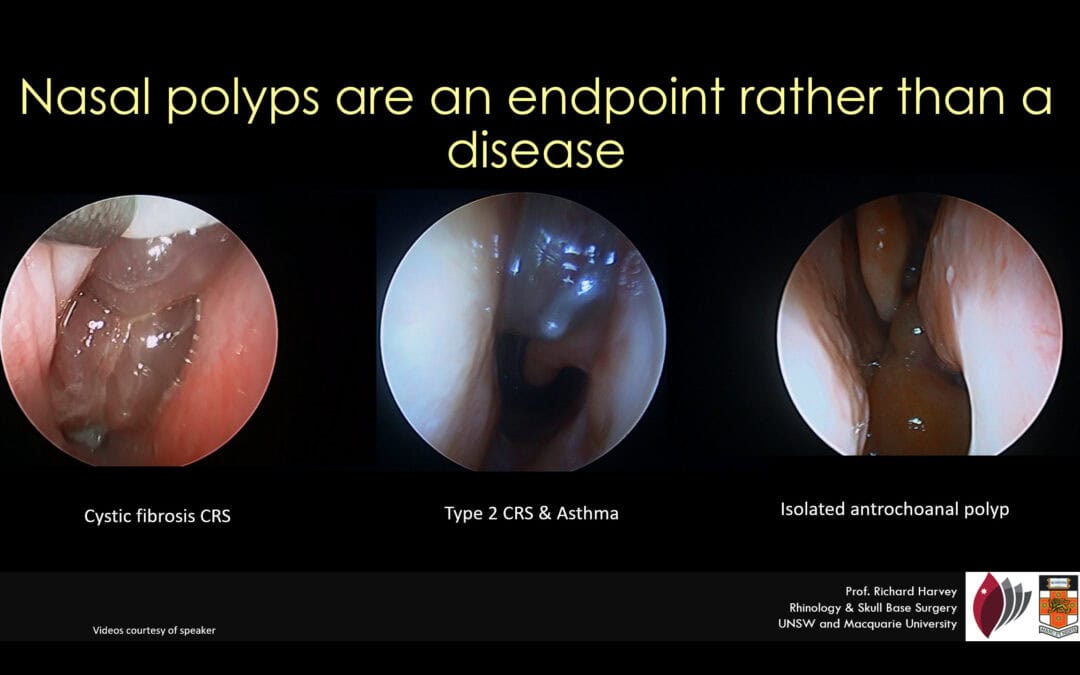
Nasal polyps are msimply the endpoint of chronic inflmmation and dont describe a specidfic disease condition
Historically, CRS was classified using a simple system:
-
CRS with nasal polyps
-
CRS without nasal polyps
While simple, this system ignores the biological diversity of sinus disease.
As research has advanced, it has become clear that these categories fail to reflect the underlying causes or mechanisms of inflammation.
Why “Nasal Polyps” Is Also a Misleading Diagnosis
The term nasal polyps is equally problematic.
A polyp is not a disease — it is a tissue response to chronic inflammation.
In other words, polyps are an endpoint of tissue remodeling, not the cause of the disease itself.
Many different conditions can produce tissue changes that look like nasal polyps.
Examples include:
-
Primary diffuse type-2 inflammatory CRS
-
Allergic fungal sinusitis (AFS)
-
Cystic fibrosis
-
Central compartment atopic disease (CCAD)
-
Respiratory epithelial adenomatoid hamartoma (REAH)
-
Antrochoanal polyps
These conditions have very different causes and treatments, yet they may all be described using the same label: “nasal polyps.”
Video:Polypoid degeneration of the sinus mucosa in cystic fibrosis. We understand that this condition wont respond to modern day biologics but then we dont discuss the ambiguity when treating non-CF CRS patients
This is why saying a patient “has nasal polyps” is often clinically incomplete.
It is similar to diagnosing someone with “a lung nodule” without explaining whether it is infection, inflammation, or cancer.
A Shift Toward Precision Medicine in Sinus Disease
Modern medicine is moving toward precision medicine — tailoring treatment based on the underlying mechanism of disease.
This approach has transformed the treatment of many inflammatory diseases, particularly asthma.
Asthma is no longer considered a single disease. Instead, it is divided into different endotypes, each driven by distinct inflammatory pathways.
The same shift is now occurring in rhinology.
Researchers and clinicians increasingly recognize that different forms of CRS require different treatments.
This is particularly important in the era of biologic therapies, including:
-
dupilumab
-
mepolizumab
-
tezepelumab
These medications target specific immune pathways and can cost tens of thousands of dollars per year.
Using them effectively requires accurate identification of the underlying disease mechanism.
The EPOS 2020 Classification of CRS
Recognising these challenges, the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS2020) proposed a more biologically meaningful classification of sinus disease.
Instead of focusing on the presence or absence of polyps, the new framework classifies primary CRS based on:
-
Anatomic distribution
-
Inflammatory endotype
This approach helps identify different clinical phenotypes that require different treatments.
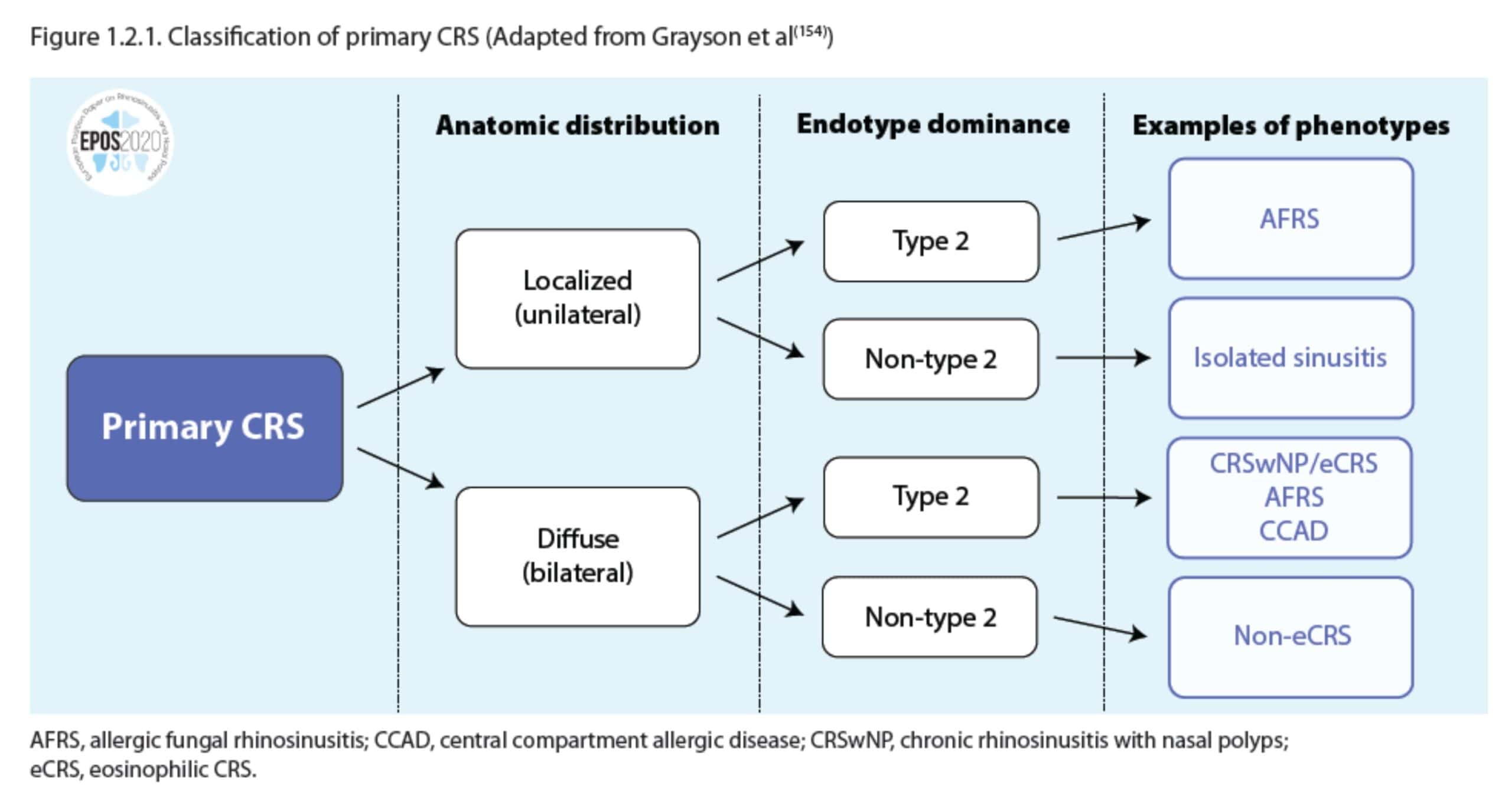
Figure: Contemporary classification of primary chronic rhinosinusitis based on anatomical distribution and inflammatory endotype, adapted from EPOS2020 and Grayson et al.
Step 1: Anatomical Distribution
Primary CRS may be divided into:
Localized disease
Examples include:
-
isolated frontal sinusitis
-
isolated sphenoid sinusitis
-
ostiomeatal complex disease
These conditions often behave more like mechanical or obstructive diseases.
Diffuse disease
Diffuse disease involves broader inflammation across the sinus system and is typically associated with systemic inflammatory pathways.
This category includes conditions such as:
-
eosinophilic CRS
-
central compartment atopic disease
-
allergic fungal sinusitis
Step 2: Inflammatory Endotype
The next layer of classification focuses on the dominant immune pathway.
Two major patterns are recognised:
Type-2 (Th2) inflammation
This pathway involves cytokines such as IL-4, IL-5, and IL-13 and is associated with:
-
eosinophilic inflammation
-
asthma
-
nasal polyps
-
corticosteroid responsiveness
Many modern biologic drugs target this pathway.
Non–Type-2 inflammation
These conditions involve different immune pathways and often behave differently clinically.
Examples include:
-
older onset disease
-
smokers
-
corticosteroid-resistant CRS
From Classification to Real Clinical Phenotypes
When anatomical distribution and inflammatory endotype are combined, a range of distinct CRS phenotypes emerges.
Examples include:
-
Central compartment atopic disease (CCAD)
-
Eosinophilic CRS (eCRS)
-
Allergic fungal sinusitis (AFS)
-
Non-eosinophilic CRS
Each has characteristic patterns of symptoms, imaging findings, and treatment responses.
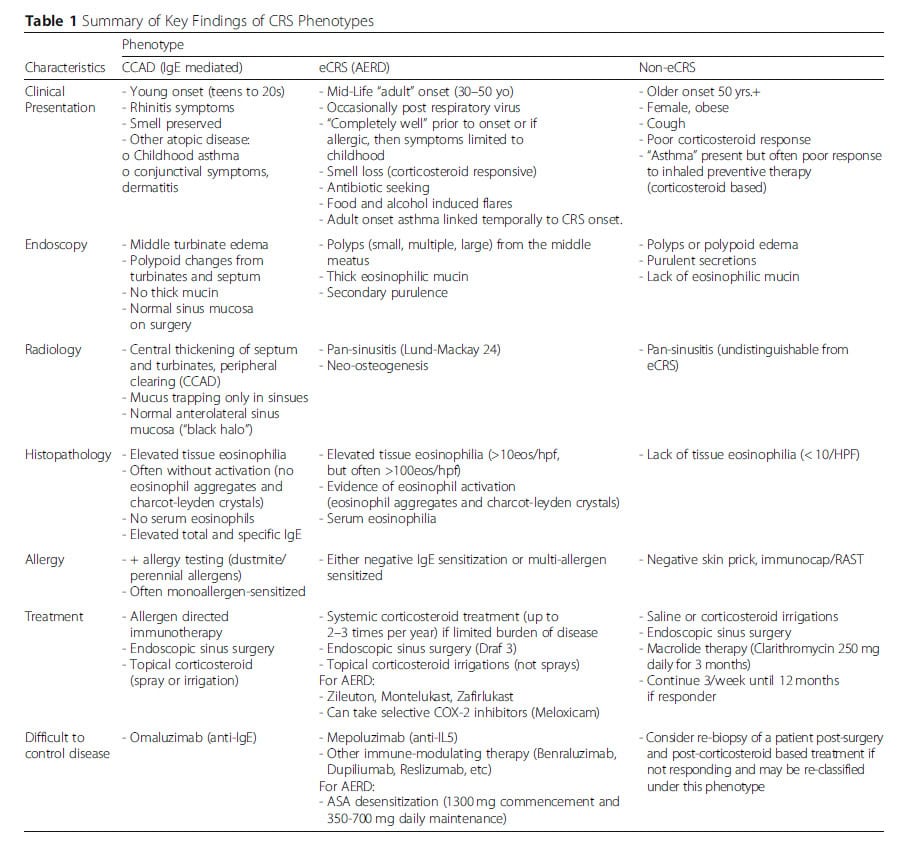
CRS is not all the same and it dictates treatment
Understanding these phenotypes allows clinicians to move beyond a simple “one size fits all” approach to sinus disease.
Why This Matters for Patients
For patients, the terminology used to describe disease can directly influence treatment decisions.
Two people diagnosed with “chronic sinusitis” may actually have completely different diseases requiring different therapies.
For example:
A patient with localized sinus obstruction may benefit primarily from surgery.
A patient with type-2 inflammatory disease may benefit from:
-
corticosteroids
-
biologic therapy
-
long-term inflammatory control.
Without recognising these differences, treatment can become trial-and-error.
Rethinking the Language of Sinus Disease
Medicine evolves as knowledge grows.
Just as asthma has evolved from a single diagnosis into multiple inflammatory subtypes, sinus disease is undergoing a similar transformation.
The terms “chronic sinusitis” and “nasal polyps” remain useful as broad descriptions, but they should not be considered final diagnoses.
Instead, they are starting points.
Behind those labels lies a complex group of conditions with distinct causes, biology, and treatments.
Recognising these differences is essential if we are to move toward precision medicine in rhinology.
And perhaps one day, the term chronic sinusitis will seem just as outdated as calling every lung disease “chronic lungitis.”
References
Frequently Asked Questions About Chronic Sinusitis
What is chronic sinusitis (CRS)?
Chronic sinusitis, also called chronic rhinosinusitis, describes persistent inflammation of the sinus lining lasting more than 12 weeks. It is not a single disease but a group of conditions with different underlying causes.
Are nasal polyps a disease?
No. Nasal polyps are not a disease themselves. They are a tissue response to chronic inflammation and can occur in many different sinus conditions.
What causes chronic sinusitis?
Many different processes can cause chronic sinus inflammation including allergy, immune dysfunction, infection, microbial imbalance, genetic diseases such as cystic fibrosis, and type-2 inflammatory conditions.
Why is CRS classification important?
Different types of CRS respond to different treatments. Understanding the underlying inflammatory pathway helps doctors choose the most effective therapy, including surgery, steroids, or biologic medications.
What is type-2 inflammation in sinus disease?
Type-2 inflammation is an immune pathway involving cytokines such as IL-4, IL-5 and IL-13. It is commonly associated with eosinophilic CRS, asthma, and nasal polyps and is the target of modern biologic therapies.
What is the EPOS classification of CRS?
The EPOS2020 guidelines classify CRS based on anatomical distribution (localized vs diffuse disease) and inflammatory endotype (type-2 vs non-type-2 inflammation).