Repairing a spontaneous nasal CSF leak in the lateral sphenoid is one of the more misunderstood operations in endoscopic skull base surgery.
At a recent national meeting, I was struck by how often panelists used the term “transpterygoid approach” while clearly describing different operations. That confusion is not trivial. It affects teaching, operative planning, and ultimately outcomes.
The issue is visible even in recent classification work. The new international sphenoid classification lists type 2C transpterygoid sphenoidotomy as “partial or complete removal of the anterior sphenoid sinus wall with partial resection of the pterygoid process”. Yet the same paper defines type 2B complete sphenoidotomy as removal of the anterior sphenoid wall extending from skull base to sphenoid floor and from septum to orbit. In practice, that means some surgeons are calling an extended sphenoid opening “transpterygoid,” (maybe vworking throguh an antrostomy) while others mean a true direct lateral transmaxillary route to the lateral recess and working lateral to the neural structures.
Those are not the same operation.
The core question should not be, “Is this transpterygoid?” The real question is:
Are we reaching a lateral defect through a direct corridor, or are we still working around corners?
Endoscopic transmaxillary / transpterygoid approach to the lateral sphenoid recess, previously via a medical maxillectomy and now done via prelacrimal. A) removal of the inferior turbinate with preservation of the inferior turbinate head, B) modified medial maxillectomy with excision of medial maxillary wall, C) removal of posterior maxillary wall, D) identification and ligation of the internal maxillary artery, E) blunt dissection through pterygopalatine and infratemporal fossa contents, F) identification of lateral pterygoid plate (arrowhead) and descending palatine nerve (arrow) which is reflected medially and preserved if possible, G) partial removal of lateral pterygoid plate and bone over lateral sphenoid recess, H) identification of meningocele defect within the lateral sphenoid recess, I) excision of meningocele and repair of defect using duragen and bone graft.
That distinction matters because most lateral sphenoid meningoceles and encephaloceles are exactly what the name suggests: lateral. In our recent prelacrimal-transmaxillary series, the defects were shown to be lateral to V2 and the foramen rotundum, and often facing laterally, which makes angled medial-to-lateral work much harder to visualize and reconstruct.
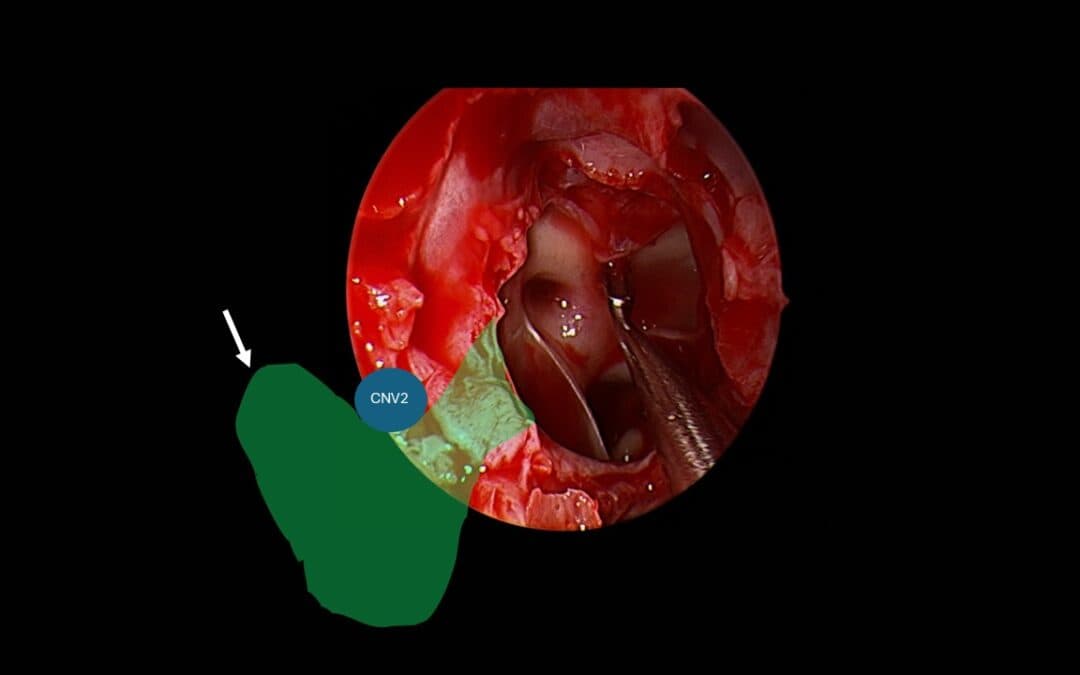
Left lateral sphenoid recess encephaloceles. Lateral to CNV2 and directed laterally. Very hard to visualize via a tranethmoid/antral approach
That is why I believe the direct route—either through a medial maxillectomy or, preferably, a prelacrimal / peri-lacrimal transmaxillary corridor—is often the most rational approach. The prelacrimal-transmaxillary technique creates a straight-line trajectory through the maxillary sinus to the posterior wall, then through the pterygoid process to the lateral sphenoid recess, allowing direct 0-degree endoscopic access and straight instruments. By contrast, the classic modified transpterygoid routes described through large antrostomies often still require surgeons to work with angled endoscopes and curved instruments “around corners”.
In our Laryngoscope technical paper, that difference is made explicit. The prelacrimal-transmaxillary approach is favored when the lateral recess is truly lateral. If the defect sits directly behind the descending root of CNV2, a wide sphenoidectomy with angled instruments may suffice. But once the defect is lateral to CNV2 and the foramen rotundum, the direct transmaxillary window is the better corridor. It also preserves the vidian bundle, the descending root of V2, and the pterygopalatine ganglion. The lateral trans-orbital root also offers access wihtout affecting these structures, but an endoscopic surgeon simply “extending” a transethmoid sphenoidectomy via an antrostomy is not.
The other concept that deserves retiring is “Sternberg’s canal”. Too often, lateral sphenoid CSF leaks are still explained as though they arise from a congenital canal in the lateral recess. That is not how I think about these patients. The defect usually behaves like an acquired weak point in a pneumatized lateral sphenoid, not a magic embryologic tunnel in the recess itself. My understanding, consistent with the position advanced by Bradford Woodworth and colleagues, is that if Sternberg’s canal exists, it is an embryologic cleft in the lateral wall of the sphenoid, not the typical lateral recess defect surgeons are closing in modern endoscopic practice.
But even that debate is secondary to the most important truth:
The hole is not the disease.
For most spontaneous lateral sphenoid CSF leaks, the underlying problem is idiopathic intracranial hypertension (IIH). The international consensus statement emphasizes that spontaneous CSF rhinorrhea is closely linked to IIH and that elevated ICP must be assessed and definitively managed after closure to avoid recurrence and long-term sequelae.
That is why we use a lumbar drain differently from many surgeons. I do not see it as a routine drain-first device. In our postoperative IIH management chapter, the preferred strategy is to clamp the lumbar drain at the end of surgery and use it to monitor ICP in the first 24 hours. If pressure is elevated, then it becomes a tool for diversion and medical decision-making. In other words, it is not there primarily to “rest” the repair. It is there to tell you whether the patient has a pressure problem that still needs treatment.
For readers who want practical numbers, the commonly used ranges are:
- Normal ICP: about 10–20 cm H₂O
- Borderline / mildly elevated: 20–25 cm H₂O
- Abnormal / consistent with raised ICP: greater than 25 cm H₂O
The consensus statement specifically supports definitive management when ICP is >25 cm H₂O. In our chapter, we also note that lumbar drains are particularly useful in higher-risk patients, including those with opening pressures >30 cm H₂O, and that persistent pressures >35 cm H₂O or poor acetazolamide response may push management toward permanent CSF diversion.
This matters because untreated IIH is not just a recurrence problem. It is also a vision problem. The consensus document recommends fundoscopy and visual assessment in these patients and stresses that long-term ICP control is needed to avoid the sequelae of untreated IIH. That is also why weight loss is critical. In our postoperative management chapter, a 6–10% reduction in weight is cited as enough to resolve IIH in some patients.In an era of GLP-1 durgs such as Ozempic, Wegovy and Monjaro, this is very achievable.
So when I look at a lateral sphenoid CSF leak, I do not think in reductionist terms.
I think:
Is the defect truly lateral?
Is my corridor direct?
Am I sparing vidian, greater palatine and Int Forum Allergy Rhinol – 2014 – Illing – Spontaneous sphenoid lateral recess cerebrospinal fluid leaks arise from ![]() V2 when I can?
V2 when I can?
And once the defect is closed, have I actually treated the disease?
Because the best repair of a lateral sphenoid leak is not just a patch.
It is the right corridor plus long-term pressure control.
FAQ
What causes a nasal CSF leak in the lateral sphenoid?
Most spontaneous lateral sphenoid CSF leaks are linked to elevated intracranial pressure rather than trauma or a simple congenital hole. The defect is often part of a broader IIH problem.
What is the best surgical approach to a lateral sphenoid CSF leak?
For truly lateral defects, a direct transmaxillary route such as a prelacrimal or medial maxillectomy corridor usually provides better access than an indirect medial route.
Is Sternberg’s canal the usual cause of lateral sphenoid CSF leak?
Probably not. The modern view is that most lateral sphenoid leaks are acquired defects related to pressure and skull base thinning rather than a classic congenital canal in the lateral recess.
Why use a lumbar drain after CSF leak repair?
In selected patients, a lumbar drain is useful as an ICP monitoring tool after closure, rather than for routine drainage. It helps determine whether additional pressure management is needed.
What ICP is considered abnormal after CSF leak repair?
Normal ICP is usually around 10–20 cm H2O. Pressures above 25 cm H2O are generally considered abnormal and may require definitive treatment.
Why is weight loss important in IIH-associated CSF leak?
Weight loss helps reduce intracranial pressure and lowers the risk of recurrence and long-term complications, including visual loss
- Ahmadzada S, Seresirikachorn K, Png LH, Campbell RG, Kalish L, Harvey RJ. Prelacrimal-transmaxillary approach to lateral sphenoid recess skull base defects. Laryngoscope. 2024.
- Georgalas C, Oostra A, Ahmed S, Castelnuovo P, Dallan I, van Furth W, et al. International consensus statement spontaneous cerebrospinal fluid rhinorrhea. Int Forum Allergy Rhinol. 2021;11(4):794-829.
- Grayson JW, Woodworth BA, Harvey RJ. 24 – Postoperative management after cerebrospinal fluid leak repair in patients with idiopathic intracranial hypertension. In: Sindwani R, Roxbury CR, editors. Cerebrospinal Fluid Rhinorrhea (First Edition). New Delhi: Elsevier; 2024. p. 161-5.
- Albaharna H, Alrasheed A, AlQahtani A, Psaltis AJ, Javer A, Meco C, et al. A novel international endoscopic sphenoid surgery classification (IESSC): a Delphi consensus. Int Forum Allergy Rhinol. 2025;15:828-836.
- Barañano CF, Curé J, Palmer JN, Woodworth BA. Sternberg’s canal: fact or fiction? Am J Rhinol Allergy. 2009 Mar-Apr;23(2):167-71. doi: 10.2500/ajra.2009.23.3290. PMID: 19401043.
- Illing E, Schlosser RJ, Palmer JN, Curé J, Fox N, Woodworth BA. Spontaneous sphenoid lateral recess cerebrospinal fluid leaks arise from intracranial hypertension, not Sternberg’s canal. Int Forum Allergy Rhinol. 2014;4:246–250.