The Septal Swell Body: The Missing Target in Nasal Obstruction Surgery
Despite decades of refinement in nasal airway surgery, one structure continues to be consistently overlooked: the septal swell body (SSB). While inferior turbinate reduction and septoplasty dominate surgical thinking, the SSB remains poorly understood, inconsistently addressed, and often misinterpreted as a simple septal deviation.
This is increasingly difficult to justify.
A growing body of anatomical, radiological, and clinical evidence now demonstrates that the SSB is not merely a structural bystander, but a dynamic, glandular, and clinically relevant contributor to nasal obstruction. Yet, many surgeons still lack a systematic approach to managing it—even in patients with persistent symptoms after otherwise adequate surgery.
More Than a Septal Thickening: A Distinct Anatomical Structure
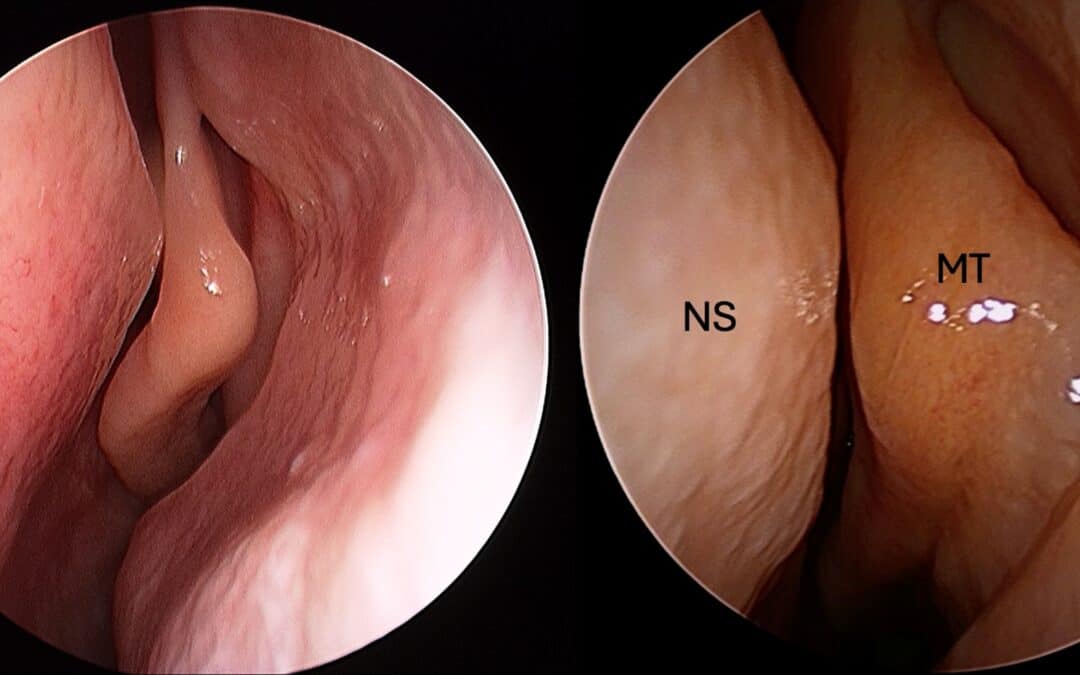
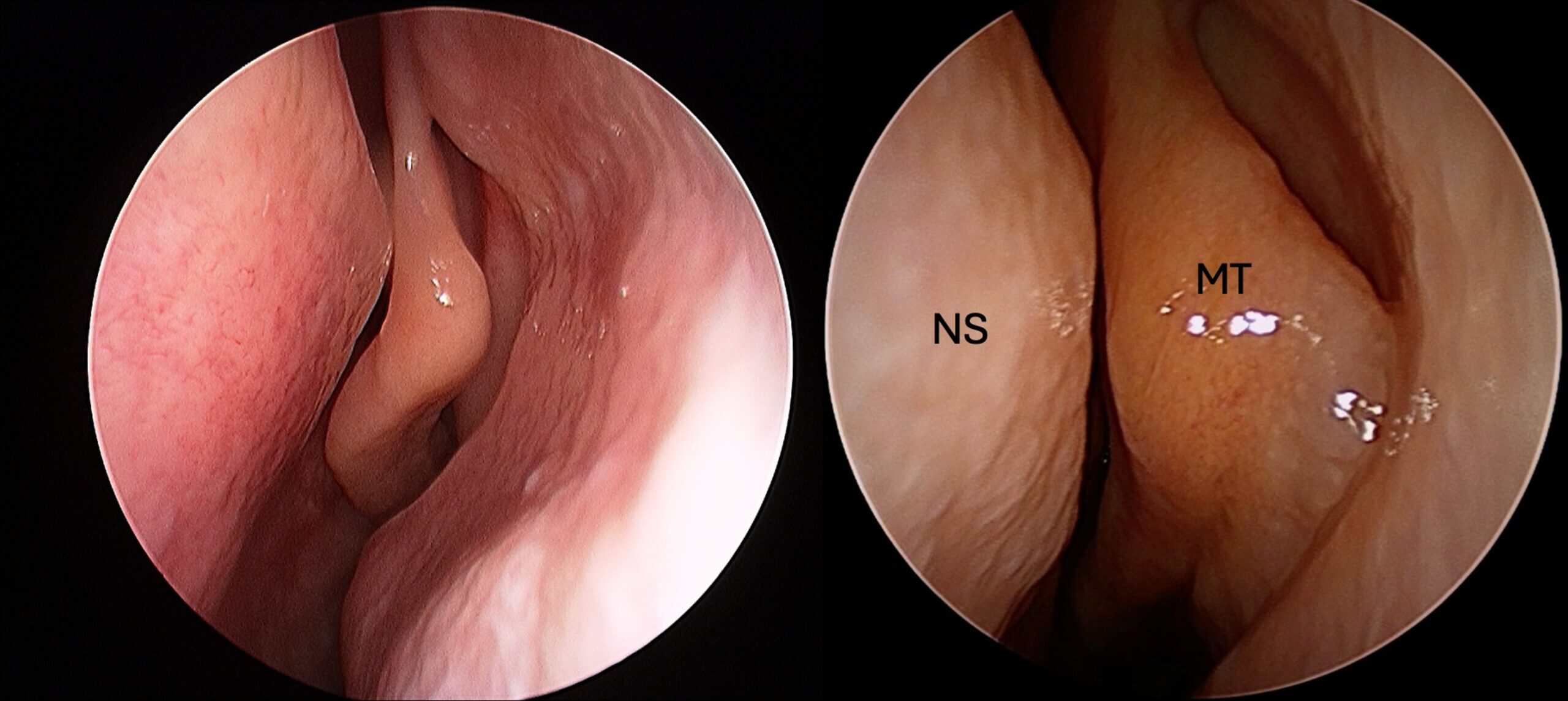
The SSB—also referred to as the nasal septal turbinate or septal body—is located anteriorly, superior to the inferior turbinate and just anterior to the middle turbinate. Importantly, it is not simply the bony-cartilaginous junction of the septum, but a fusiform, soft tissue structure with substantial mucosal volume .
Histologically, it is markedly different from the surrounding septum. Studies consistently show that the SSB contains:
- abundant seromucinous glands (~50%)
- venous sinusoids and erectile tissue
- thickened mucosa with vascular capacity
This composition closely resembles inferior turbinate tissue rather than septal mucosa .
This distinction is critical. It reframes the SSB as a functional structure, capable of active physiological change, rather than a passive anatomical variant.
A Dynamic Contributor to Nasal Airflow
The SSB behaves like a turbinate.
Radiological evidence demonstrates that it is dynamic in size, with measurable changes over time that correlate directly with inferior turbinate variation. In a longitudinal CT-based study, changes in SSB width significantly correlated with turbinate size changes (r = 0.35, p = 0.04), supporting a shared role in nasal cycling and airflow regulation .
This has practical implications:
- Enlargement of the SSB contributes to internal nasal valve narrowing
- It increases nasal airway resistance
- It participates in the nasal cycle alongside turbinates
Despite this, most surgical paradigms still focus almost exclusively on the lateral wall.
Hypertrophy in Disease: Allergy and Inflammation
The SSB is not static—it responds to disease.
Multiple radiographic studies demonstrate that the SSB is significantly enlarged in patients with sinonasal disease, particularly those with allergic rhinitis and turbinate hypertrophy.
In a large CT-based study of 405 patients:
- SSB dimensions were significantly greater in diseased vs control groups
- For example, middle segment thickness: 12.74 mm vs 10.47 mm (p=0.001)
Similarly, Hizli et al. demonstrated that:
- SSB size is significantly larger in patients with inferior turbinate hypertrophy
- Allergy has an additive effect, further increasing SSB area and width (p < 0.001)
This reinforces a key concept:
The septal swell body undergoes the same inflammatory hypertrophy as the inferior turbinate
Yet, while turbinate hypertrophy is routinely treated, SSB hypertrophy is often ignored.
The septal swell body or septal turbinate undergoes the same tissue remodelling as the IT.
The Evidence for Treatment: Not Just Theory
The most compelling argument for addressing the SSB is clinical outcomes.
A recent systematic review and meta-analysis (2025) evaluated septal swell body volume reduction (SSBVR) across seven studies (n=232 patients). The findings were clear:
- Significant improvement in nasal obstruction scores (SMD 2.54)
- Reduction in nasal airway resistance (SMD –0.67)
- Increased cross-sectional area (SMD –1.05)
- Benefits sustained up to 12 months
Perhaps more importantly:
Adding SSB reduction to turbinate surgery improved outcomes compared to turbinate surgery alone (SMD 0.47)
This directly challenges current surgical practice.
If turbinate surgery alone is inferior, then failing to address the SSB may represent incomplete surgery.
Why Is the SSB Still Ignored?
Despite this growing evidence, many surgeons do not routinely treat the SSB.
There are several reasons:
- Misidentification as septal deviation
- Lack of emphasis during surgical training
- Perception that intervention is unnecessary or risky
- Absence of consensus guidelines
A systematic review of the nasal septal turbinate concluded that it remains an “overlooked surgical target”, despite consistent anatomical and early clinical evidence supporting its relevance .
This aligns with real-world experience. Many international observers—across Europe, Asia, and South America—report no exposure to SSB surgery during training, highlighting a global gap in rhinologic education.
Safety: Addressing a Common Concern
One concern often raised is the risk of septal perforation.
However, this appears overstated.
Across intervention studies:
- Procedures are typically performed bilaterally
- Reported complication rates are very low (~1–2%)
- Septal perforation rates remain rare (<2%)
This reflects both:
- preservation of underlying septal support
- mucosal-sparing techniques
In practice, SSB reduction is no more hazardous than turbinate surgery, when performed correctly.
Surgical Relevance: Beyond Nasal Obstruction
The importance of the SSB extends beyond symptom control.
In endoscopic sinus surgery, particularly:
- access to the middle meatus
- instrumentation of the osteomeatal complex
the SSB can act as a medial barrier, limiting exposure.
Failure to address it can:
- restrict surgical access
- compromise visualization
- reduce completeness of surgery
Thus, SSB management is not only about improving airflow—it is also about optimising surgical corridors.
A Balanced Approach: Treat the Disease, Not Just the Anatomy
While surgical management is important, it must be contextualised within overall disease control.
The SSB is particularly responsive to:
- allergic inflammation
- chronic rhinosinusitis
Therefore:
- allergen immunotherapy (AIT)
- medical optimisation
remain essential components of care.
Surgery should be viewed as:
an adjunct to disease control—not a replacement for it
A Call for Change in Surgical Thinking
The evidence is now difficult to ignore.
The septal swell body is:
- histologically distinct
- functionally dynamic
- responsive to inflammation
- clinically relevant in obstruction
- supported by outcome data when treated
And yet, it remains inconsistently addressed.
This represents a gap between evidence and practice.
Conclusion
Modern rhinology is moving toward precision—targeting specific structures based on function, pathology, and outcomes.
The septal swell body fits squarely within this paradigm.
Ignoring the septal swell body in nasal obstruction surgery risks incomplete treatment.
For surgeons, this is an opportunity to refine technique and improve outcomes.
For patients, it represents a shift toward more comprehensive, physiology-based care.
References
- Kim JS, Stybayeva G, Hwang SH. Effectiveness of septal swell body reduction for patients with nasal airway obstruction: a systematic review and meta-analysis. Clin Exp Otorhinolaryngol. 2025;18(2):171–179.
- Gelera JE, Ojar D, Lim JH, et al. Radiographic changes of the nasal septal body among patients with sinonasal diseases. Clin Exp Otorhinolaryngol. 2017;10(4):338–343.
- Hizli O, Kayabasi S, Ozkan D. Is nasal septal body size associated with inferior turbinate hypertrophy and allergic rhinitis? J Craniofac Surg. 2020;31:778–781.
- Wong EH, Noussair M, Hasan Z, et al. Physiological changes in the size of the septal swell body correlate with changes in inferior turbinate size. J Laryngol Otol. 2020;134:323–327.
- Moss WJ, Faraji F, Jafari A, DeConde AS. A systematic review of the nasal septal turbinate: an overlooked surgical target. Am J Otolaryngol. 2019;40(6):102188.
- Patrascu E, Budu V, Musat G. Nasal swell body: a literature review. Rom J Rhinol. 2020;10(37):19–24.
FAQs
What is the septal swell body?
The septal swell body is a gland-rich, vascular structure on the nasal septum that contributes to airflow regulation and nasal resistance.
Can the septal swell body cause nasal obstruction?
Yes. Enlargement of the septal swell body—especially in allergy or chronic inflammation—can significantly contribute to nasal blockage.
Why is the septal swell body often not treated?
It is frequently mistaken for septal deviation or overlooked during training, so many surgeons do not routinely address it.
Does treating the septal swell body improve outcomes?
Yes. Studies show that treating it alongside turbinate surgery improves nasal obstruction symptoms compared to turbinate surgery alone.
Is septal swell body surgery safe?
Yes. Complication rates are low, with studies showing less than 2% risk of issues such as bleeding or septal perforation.