
Achieving a bloodless surgical field in endoscopic sinus surgery
Why the surgical field matters in sinus surgery
Endoscopic sinus surgery is performed through narrow corridors, close to the orbit, skull base, optic nerve, carotid artery and anterior ethmoidal artery. In this environment, bleeding is not just an inconvenience. It degrades orientation.
A poor field makes it harder to recognise anatomical landmarks, identify sinus outflow pathways, complete the operation efficiently and avoid complications. It may also increase postoperative scarring and the risk of incomplete surgery. These principles have been central to rhinology teaching for decades: haemostasis affects visibility, operative time, completeness of surgery and the surgeon’s ability to stay oriented during dissection.
The aim is not simply to reduce the number of millilitres of blood loss. A case can have modest total blood loss but still have a poor endoscopic field if there is persistent mucosal ooze across the lens and operative target. The real goal is a quiet field where anatomy remains visible and decisions remain precise.
This is why many rhinologists use the Boezaart scale, also known as the Fromme-Boezaart scale, to describe intraoperative bleeding. It is a 0-to-5 surgical field scale in which 0 represents no bleeding and 5 represents severe bleeding that prevents surgery. It was popularised in endoscopic sinus surgery by Boezaart and colleagues in their comparison of sodium nitroprusside- and esmolol-induced controlled hypotension for functional endoscopic sinus surgery.¹
A movement from a Boezaart 3 or 4 field to a Boezaart 1 or 2 field is not a small change. It is often the difference between repeatedly suctioning blood and being able to operate deliberately.
A bloodless field is built in layers
No single manoeuvre reliably creates the ideal field. The best results come from stacking several modest but evidence-supported interventions:
- early topical vasoconstriction and local mucosal injection
- reverse Trendelenburg positioning
- perioperative tranexamic acid
- bradycardic, carefully controlled anaesthesia
- mucosal-preserving surgical technique
Each component may improve the surgical field by a modest amount. Across the operation, the cumulative difference can be large. It is reasonable to think of many of these interventions as moving the field by roughly half a Boezaart grade or more, depending on the patient and disease process.
That is not a formal mathematical equation. The trials do not prove simple additivity across all interventions. But clinically, the cumulative effect is obvious. A case performed flat, with inhalational anaesthesia, no tranexamic acid, late or weak vasoconstriction and mucosal stripping is a different operation from one performed with a complete haemostatic strategy.
1. Start early: topical vasoconstriction and local mucosal injection
The nose is highly vascular. The sinonasal mucosa contains resistance vessels, capacitance vessels, venous sinusoids and mucosal microvasculature. Effective vasoconstriction needs to start before the first incision or instrument trauma.
Our principle is early application of high-concentration, non-selective alpha agonist vasoconstriction, most commonly topical adrenaline / epinephrine where appropriate. The rationale is that alpha-1 activity constricts resistance vessels, while alpha-2 activity contributes to venous capacitance vessel constriction. By contrast, partial alpha agonists such as oxymetazoline and phenylephrine are useful decongestants but may produce less complete mucosal vasoconstriction than adrenaline-based preparation.²
In our practice, topical preparation commonly uses 1:2000 adrenaline with 1% ropivacaine. This is applied early and allowed time to work. Topical preparation remains the most important local step because it treats a broad mucosal surface before bleeding has started.
For clarity, 1:2000 adrenaline is equivalent to 0.5 mg/mL adrenaline. 1% ropivacaine is equivalent to 10 mg/mL ropivacaine. These concentrations require local institutional approval, anaesthetic awareness and disciplined use. The purpose of providing the details is to describe a reproducible rhinology workflow, not to replace local medication governance.
Local mucosal injection is then used as a second step, not as a substitute for topical preparation. A typical 10 mL syringe mixture is:
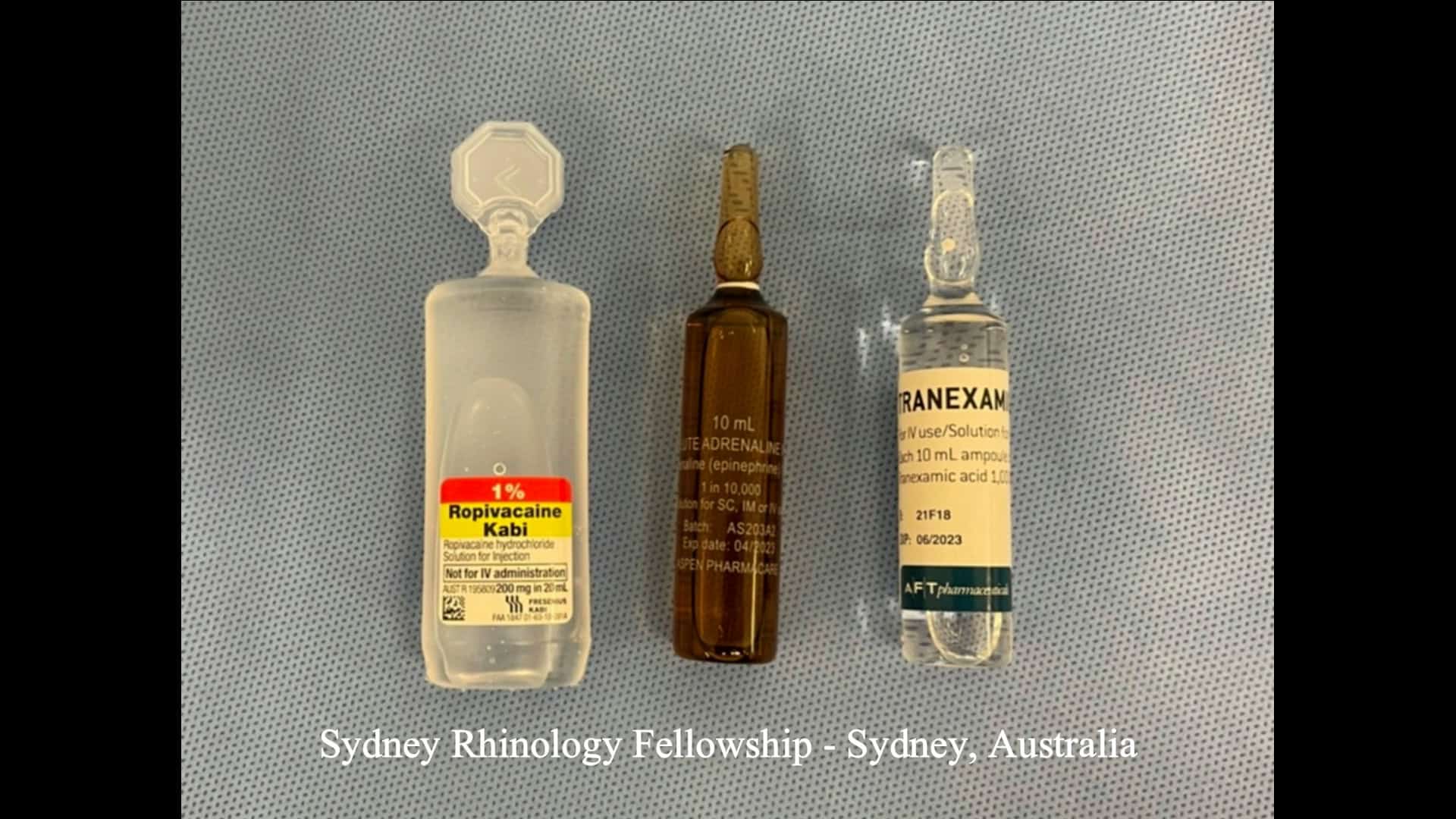
8 mL of 1% ropivacaine
1 mL of 1:10,000 adrenaline
1 mL of tranexamic acid, using 1 mL from a 1000 mg / 10 mL ampoule, equivalent to 100 mg TXA
This gives a final 10 mL solution containing:
- ropivacaine: 80 mg total, or 8 mg/mL, equivalent to 0.8%
- adrenaline: 0.1 mg total, or 10 micrograms/mL, equivalent to 1:100,000
- tranexamic acid: 100 mg total, or 10 mg/mL, equivalent to 1%
The raw ingredients are often more useful to surgeons than the final concentrations because they allow the mixture to be replicated consistently within local pharmacy and anaesthetic governance. The dose still needs to be checked against patient weight, cardiovascular risk, renal function, maximum local anaesthetic dosing, anticoagulant status and institutional protocols.
Topical adrenaline in nasal surgery has been studied for systemic catecholamine effects. Van Hasselt and colleagues compared plasma catecholamine levels after topical application versus infiltration of adrenaline for nasal surgery.³ The practical point is not that topical adrenaline is risk-free; it must be used with appropriate anaesthetic communication, dosing discipline and cardiovascular awareness. But when used correctly, it remains one of the most effective tools for mucosal preparation.
The sequence also matters. If a weaker partial agonist is applied first, there is a theoretical risk of occupying receptors before a stronger non-selective vasoconstrictor is used. This is one reason many high-volume rhinology units standardise preparation rather than relying on ad hoc topical sprays immediately before surgery.
2. Position: reverse Trendelenburg is not cosmetic
Positioning is one of the simplest and most underused interventions for surgical field quality.
A 15- to 20-degree reverse Trendelenburg position reduces venous congestion and improves the endoscopic field. Hathorn and colleagues randomised patients undergoing FESS to 15-degree reverse Trendelenburg or horizontal positioning and concluded that the 15-degree reverse Trendelenburg position improved the field of view and reduced blood loss.⁴ Gan and colleagues later studied 5-, 10- and 20-degree reverse Trendelenburg positioning in a double-blind randomised controlled trial.⁵
The mechanism is straightforward. Head-up positioning lowers venous pressure in the operative field. In prior surgical teaching material, reverse Trendelenburg positioning is highlighted as reducing central venous pressure and nasal mucosal blood flow. The practical clinical effect is that less venous congestion is delivered into the operative field.

Ideal positioning for hemostatic control is 15-20deg and appears more than expected. simple iphone utilities help with inital judgement
The important clarification is that reverse Trendelenburg is not the same as dangerous cerebral hypoperfusion. A 15- to 20-degree head-up position is generally well tolerated under modern anaesthesia, with the anaesthetist maintaining appropriate cerebral perfusion and systemic parameters. The aim is controlled venous unloading, not extreme hypotension.
In practical terms, this is often the single easiest improvement to implement. If the patient is flat, the surgeon is already accepting avoidable venous congestion.
3. Tranexamic acid: antifibrinolysis for a better field
Tranexamic acid is a synthetic lysine analogue that inhibits fibrinolysis by blocking plasminogen binding to fibrin. It stabilises clot rather than causing vasoconstriction.⁶
For endoscopic sinus surgery, the strongest current evidence is the 2023 Cochrane review by Lourijsen and colleagues. It included 14 randomised controlled trials with 942 participants. Tranexamic acid, administered topically or intravenously, probably reduced surgical field bleeding score, with a standardised mean difference of -0.87 using Boezaart or Wormald grading systems. It also reduced intraoperative blood loss by a mean of 70.32 mL and reduced operative time by about 13 minutes. No seizures or thromboembolic events were reported within 24 hours in the included studies, although longer-term adverse-event data were limited.⁷
The usual perioperative dose used in many sinus surgery studies is approximately 10–15 mg/kg intravenously at induction, commonly translating to about 1000 mg in an adult. This should still be individualised for renal function, thrombotic history and local anaesthetic protocols.
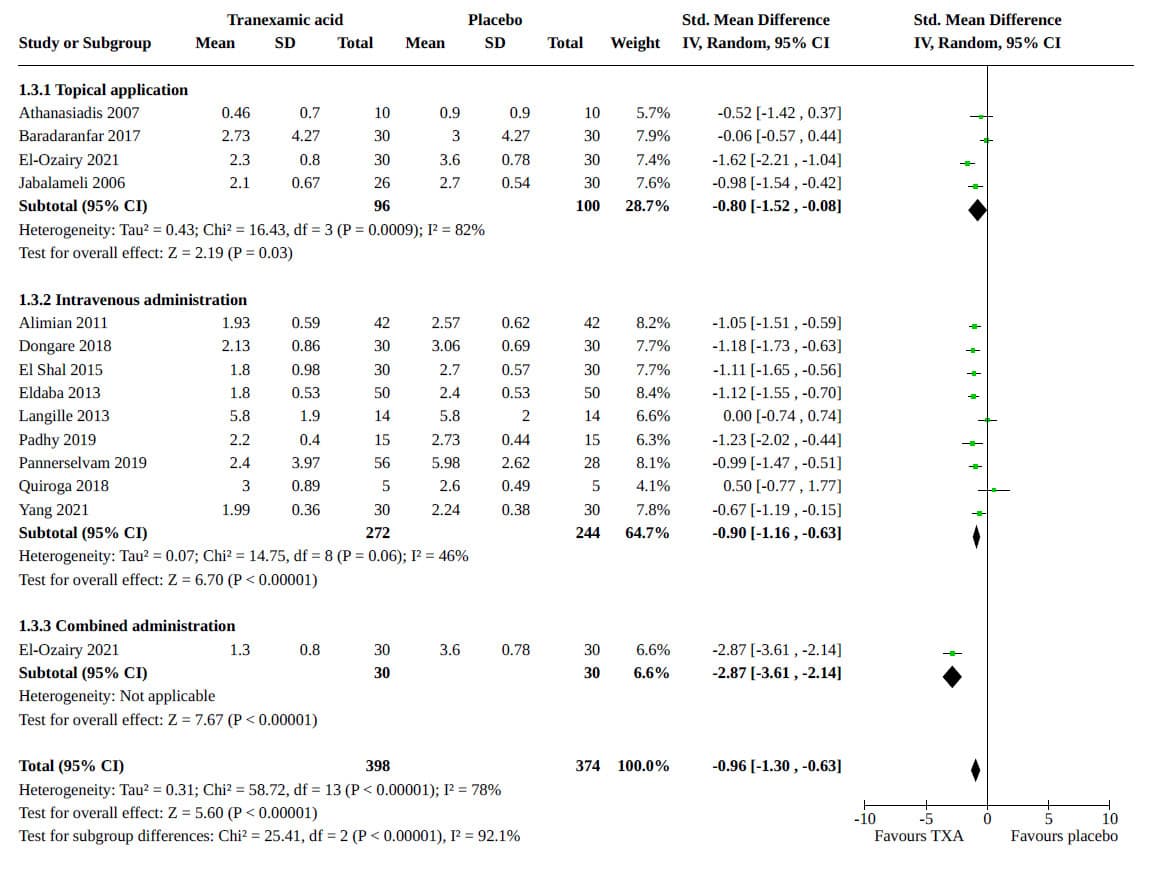
The pooled result demonstrated that tranexamic acid probably reduces the surgical field bleeding score, with a standardised mean diHerence (SMD) of -0.87 (95% confidence interval (CI) -1.23 to -0.51; 13 studies, 772 participants; moderate-certainty evidence). A SMD below -0.70 represents a large eHect (in either direction).
The safety profile of intravenous tranexamic acid has also been examined beyond rhinology. Taeuber and colleagues analysed 216 randomised trials involving 125,550 patients and found no association between intravenous tranexamic acid and increased overall thromboembolic events; events occurred in 2.1% of TXA patients versus 2.0% of controls.⁸ That does not remove the need for case selection, but it counters the common reflex that TXA is inherently unsafe.
The practical message is simple: tranexamic acid is cheap, pharmacologically rational and supported by sinus surgery-specific Cochrane evidence.
4. Anaesthesia: hypotension is not the whole goal
The old phrase “hypotensive anaesthesia” can be misleading. In sinus surgery, the goal is not simply to push the blood pressure as low as possible. The field is influenced by cardiac output, heart rate, venous pressure, mucosal vasodilation, anaesthetic technique and local surgical trauma.
A more accurate target is often bradycardic, mildly hypotensive, low-flow physiology under carefully monitored anaesthesia.
Total intravenous anaesthesia, particularly propofol-remifentanil-based techniques, has repeatedly shown advantages in surgical field visibility compared with inhalational anaesthesia. Kolia and Man’s 2019 meta-analysis of randomised trials found TIVA superior to inhalational anaesthesia for visual field, estimated blood loss and operative time.⁹ Moffatt and colleagues’ 2021 meta-analysis similarly found that TIVA had superior intraoperative visibility scores and blood loss compared with inhalational anaesthesia.¹⁰
There is also Cochrane-level evidence that deliberate hypotension with propofol can improve the surgical field in FESS.¹¹ But the nuance matters: hypotension without control of heart rate and venous congestion is not the same as a good endoscopic field. Esmolol-based approaches in the original Boezaart work are relevant because they emphasise the importance of heart rate and flow, not merely arterial pressure.¹
The anaesthetic plan should therefore be discussed before the case begins. The surgeon and anaesthetist should agree on the field objective, expected complexity, acceptable haemodynamic range and whether TIVA, remifentanil, beta-blockade or other approaches are appropriate for the patient.
5. Technique: do not create bleeding that drugs cannot fix
The final step is surgical discipline.
Vasoconstrictors work on smooth-muscle-containing vessels. They do not solve bleeding from stripped mucosa, exposed cancellous bone or bony Haversian channels. Once mucosa is avulsed and raw bone is exposed, the surgeon has created a bleeding surface that is less responsive to topical vasoconstriction.
The principle is simple: preserve mucosa wherever possible.
This means biting rather than pulling, using through-cutting forceps correctly, avoiding mucosal stripping, using the microdebrider in a controlled fashion, maintaining a clean suction tip, and respecting tissue planes. In prior teaching material, the surgical message was deliberately blunt: “No stripping of mucosa” and “mucosa-bone-mucosa.”
This is not just aesthetic surgical technique. It is haemostatic technique. A surgeon who strips mucosa creates their own bleeding problem and then blames the anaesthetist.
What the Boezaart scale teaches us
The Boezaart scale is useful because it converts a subjective frustration into a shared operative language. A one-point difference is clinically meaningful. A two-point difference is major.
The evidence for any individual intervention is often modest: a better field with reverse Trendelenburg, a better field with TIVA, a better field with tranexamic acid, a better field with proper vasoconstriction and careful technique. But in real surgery these do not occur in isolation. They stack.
The goal is not to perform surgery in a dry-looking field for cosmetic satisfaction. The goal is orientation. The cleaner the field, the easier it is to identify the skull base, lamina papyracea, frontal recess, sphenoid face, posterior ethmoid partitions and vascular landmarks.
That is the difference between operating on anatomy and operating through blood.
Patient factors still matter
Not every case can be made bloodless. Severe eosinophilic polyposis, active infection, fungal disease, revision surgery, anticoagulation, hypertension, vascular tumours and distorted anatomy all increase bleeding risk.
Preoperative medical optimisation may help in selected patients, particularly those with nasal polyposis. Earlier evidence syntheses have suggested that preoperative steroids may improve blood loss, operative time and surgical field grade in polyp surgery, although this needs to be balanced against the goal of preserving tissue for biopsy, histology and endotyping in modern CRS care.¹²
A bloodless field is therefore not simply an anaesthetic trick or a drug protocol. It starts with correct patient selection, control of inflammation where appropriate and knowing what disease process is being operated on.
Why patients should care
Patients do not usually ask about Boezaart scores. They ask whether surgery will be safe and effective.
A clear surgical field contributes directly to that. It allows the surgeon to see the skull base, orbit, lamina papyracea, frontal recess, sphenoid face, posterior ethmoid partitions and vascular landmarks. It helps the surgeon complete the planned dissection rather than stopping early because the field is unsafe. It reduces unnecessary trauma and may reduce operative time.
For surgeons, the surgical field is a technical outcome. For patients, it is a safety outcome.
What about PPF injections?
Pterygopalatine fossa injection can be a useful adjunct in selected sinus surgery cases, but it is not required in every operation and should not be presented as one of the core five steps.
The injection is performed by infiltration through the greater palatine canal, targeting the pterygopalatine fossa region. It is sometimes loosely referred to as a “PPF injection,” but the practical route is the greater palatine canal.
We use this selectively when initial topical vasoconstriction or local mucosal injection is difficult, such as in patients with a very large polyp load, obstructing inflammatory disease or selected vascular tumour cases. In these situations, the early field can be poor before the surgeon has adequate access to place topical patties or perform precise local infiltration.
There is evidence supporting both haemostatic and analgesic benefit. Hwang and colleagues’ systematic review and meta-analysis found that greater palatine canal injections with local anaesthetic and vasoconstrictor reduced operative bleeding during endoscopic sinus surgery.¹³ A separate meta-analysis of sphenopalatine block in endoscopic sinus surgery found reductions in intraoperative bleeding, postoperative pain, nausea and vomiting, and recovery from sedation, without significant adverse effects in the included studies.¹⁴
The technique is demonstrated in this prior teaching video:
This video uses the phrase “PPF canal,” but anatomically the injection is performed through the greater palatine canal to access the pterygopalatine fossa region. The technique should be framed as an adjunct, not a replacement for the core haemostatic strategy. The main pillars remain topical vasoconstriction, reverse Trendelenburg positioning, tranexamic acid, appropriate anaesthesia and mucosal-preserving surgical technique.
The practical recipe
A reproducible approach to endoscopic sinus surgery haemostasis is:
- prepare the mucosa early with effective topical vasoconstriction
- use local mucosal injection when appropriate
- place the patient in 15–20 degrees reverse Trendelenburg
- consider perioperative tranexamic acid, commonly 10–15 mg/kg or about 1 g IV, where not contraindicated
- use TIVA and aim for controlled bradycardic, mildly hypotensive physiology rather than crude hypotension alone
- preserve mucosa and avoid exposing raw bone unnecessarily
- consider greater palatine canal / pterygopalatine fossa injection as an adjunct in selected cases where early topical or local access is difficult
The best field is not achieved by one heroic manoeuvre. It is achieved by making several sensible decisions before and during every case.
A bloodless field is not about making surgery look elegant. It is about making endoscopic sinus surgery safer, more efficient, more complete and more anatomically controlled..
Related articles
Chronic rhinosinusitis
https://richardharvey.sydneyentclinic.com/2022/02/12/do-i-really-have-sinusitis-chronic-sinus-symptoms/
References
- Boezaart AP, van der Merwe J, Coetzee A. Comparison of sodium nitroprusside- and esmolol-induced controlled hypotension for functional endoscopic sinus surgery. Can J Anaesth. 1995;42(5 Pt 1):373–376. doi:10.1007/BF03015479.
- Corboz MR, Rivelli MA, Varty L, Mutter J, Cartwright M, Rizzo CA, et al. Pharmacological characterization of postjunctional alpha-adrenoceptors in human nasal mucosa. Am J Rhinol. 2005;19(5):495–502.
- van Hasselt CA, Low JM, Waldron J, Gibb AG, Oh TE. Plasma catecholamine levels following topical application versus infiltration of adrenaline for nasal surgery. Anaesth Intensive Care. 1992;20(3):332–336. doi:10.1177/0310057X9202000310.
- Hathorn IF, Habib AR, Manji J, Javer AR. Comparing the reverse Trendelenburg and horizontal position for endoscopic sinus surgery: a randomized controlled trial. Otolaryngol Head Neck Surg. 2013;148(4):608–613. doi:10.1177/0194599812466529.
- Gan EC, Habib AR, Rajwani A, Javer AR. Five-degree, 10-degree, and 20-degree reverse Trendelenburg position during functional endoscopic sinus surgery: a double-blind randomized controlled trial. Int Forum Allergy Rhinol. 2014;4(1):61–68. doi:10.1002/alr.21249.
- Ockerman A, Vanassche T, Garip M, Vandenbriele C, Engelen MM, Martens J, et al. Tranexamic acid for the prevention and treatment of bleeding in surgery, trauma and bleeding disorders: a narrative review. Thromb J. 2021;19:54. doi:10.1186/s12959-021-00303-9.
- Lourijsen E, Avdeeva K, Gan KL, Pundir V, Fokkens W. Tranexamic acid for the reduction of bleeding during functional endoscopic sinus surgery. Cochrane Database Syst Rev. 2023;2:CD012843. doi:10.1002/14651858.CD012843.pub2.
- Taeuber I, Weibel S, Herrmann E, Neef V, Schlesinger T, Kranke P, Messroghli L, et al. Association of intravenous tranexamic acid with thromboembolic events and mortality: a systematic review, meta-analysis, and meta-regression. JAMA Surg. 2021;156(6):e210884. doi:10.1001/jamasurg.2021.0884.
- Kolia NR, Man LX. Total intravenous anaesthesia versus inhaled anaesthesia for endoscopic sinus surgery: a meta-analysis of randomized controlled trials. Rhinology. 2019;57(6):402–410. doi:10.4193/Rhin19.168.
- Moffatt DC, McQuitty RA, Wright AE, Kamucheka TS, Haider AL, Chaaban MR. Evaluating the role of anesthesia on intraoperative blood loss and visibility during endoscopic sinus surgery: a meta-analysis. Am J Rhinol Allergy. 2021;35(5):674–684. doi:10.1177/1945892421989155.
- Boonmak P, Boonmak S, Laopaiboon M. Deliberate hypotension with propofol under anaesthesia for functional endoscopic sinus surgery. Cochrane Database Syst Rev. 2016;10:CD006623. doi:10.1002/14651858.CD006623.pub3.
- Pundir V, Pundir J, Lancaster G, Baer S, Kirkland P, Cornet M, et al. Role of corticosteroids in functional endoscopic sinus surgery: a systematic review and meta-analysis. Rhinology. 2016;54(1):3–19. doi:10.4193/Rhino15.079.
- Hwang SH, Kim SW, Kim SW, Kim BG, Cho JH, Kang JM. Greater palatine canal injections reduce operative bleeding during endoscopic sinus surgery: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 2019;276(1):3–10. doi:10.1007/s00405-018-5138-6.
- Kim DH, Kang H, Hwang SH. The effect of sphenopalatine block on the postoperative pain of endoscopic sinus surgery: a meta-analysis. Otolaryngol Head Neck Surg. 2019;160(2):223–231. doi:10.1177/0194599818805673.
FAQ section for the page
FAQ
Why does bleeding matter in endoscopic sinus surgery?
Bleeding matters because endoscopic sinus surgery is performed close to the orbit, skull base, optic nerve and major blood vessels. Even modest bleeding can obscure landmarks, reduce surgical orientation and make the procedure less efficient or less complete.
What is the Boezaart scale?
The Boezaart scale, also called the Fromme-Boezaart scale, is a 0-to-5 grading system used to describe intraoperative bleeding and the quality of the surgical field during endoscopic sinus surgery. A lower score means a clearer field.
What helps create a clearer field during sinus surgery?
A clearer field is usually achieved by combining several steps: early topical vasoconstriction, local mucosal injection, reverse Trendelenburg positioning, tranexamic acid, carefully controlled anaesthesia and mucosal-preserving surgical technique.
Why is reverse Trendelenburg positioning used in sinus surgery?
Reverse Trendelenburg positioning places the patient slightly head-up, often around 15 to 20 degrees. This reduces venous congestion in the nose and sinuses, which can improve the surgical field without relying only on lowering blood pressure.
What is tranexamic acid used for in endoscopic sinus surgery?
Tranexamic acid is an antifibrinolytic medication. It helps stabilise clot formation and has been shown in systematic reviews to improve surgical field bleeding scores, reduce blood loss and modestly reduce operative time in endoscopic sinus surgery.
Is hypotension the main goal of anaesthesia for sinus surgery?
No. The goal is not simply to make the blood pressure as low as possible. A better target is controlled bradycardic, mildly hypotensive physiology with low venous congestion and stable cerebral perfusion. TIVA techniques often help achieve this.
What is a pterygopalatine fossa injection?
A pterygopalatine fossa injection is an adjunctive technique performed through the greater palatine canal. It may assist with haemostasis and analgesia in selected cases, especially when topical vasoconstriction or local injection is difficult because of large polyps or tumour bulk.
Why does mucosal-preserving technique reduce bleeding?
Vasoconstrictors work best on smooth-muscle-containing vessels. If mucosa is stripped and raw bone is exposed, bleeding may come from bony channels that are less responsive to vasoconstriction. Preserving mucosa reduces avoidable bleeding.