Nose Picking, Crusting and Septal Perforations: The Missing Part of the Story
Nose picking is one of the most common human behaviours that almost nobody wants to discuss honestly. In most people, it is harmless. It is not a disease, and it is not automatically a psychiatric problem. It is usually just a way of clearing dried mucus from the nose.
In rhinology, however, the subject matters.
For years, many surgeons were taught that chronic septal crusting, septal ulceration and septal perforation were mainly explained by drying from nasal airflow. That explanation is partly true. The nose conditions a large volume of air every day. Depending on activity, climate and physiology, roughly 15,000–20,000 litres of air may pass through the nasal cavity in a day. Airflow can dry secretions, thicken mucus, and contribute to crusting.
But airflow is not the whole story.
In many patients, the missing mechanical factor is the finger. A crust forms, the patient feels blocked, they clear it, the surface bleeds or becomes raw, a new crust forms, and the cycle repeats. The patient is not being “bad”. They are often trying to breathe. The problem is that the wound surface is being reset every day.
Nose picking: normal behaviour versus a medical problem
The medical term often used for compulsive nose picking is rhinotillexomania. That term is useful, but it can also confuse the discussion. Most people who pick their nose do not have rhinotillexomania.
The available survey data make this clear. Jefferson and Thompson’s adult survey reported that nose picking was an almost universal adult behaviour and concluded that, in most people, it should be regarded as a habit rather than a psychiatric disorder.[1] A later adolescent survey found that almost the entire adolescent sample admitted to nose picking, with a median frequency of four times per day. In that study, 7.6% reported picking more than 20 times per day, and nearly 17% considered that they had a serious nose-picking problem.[2]
The practical distinction is therefore important:
- Common nose picking is occasional clearing of dried mucus or crust.
- Clinically relevant nose picking is repeated mechanical trauma to vulnerable nasal mucosa.
- Rhinotillexomania is compulsive, repetitive picking that may be difficult to control and may require behavioural or psychological support.
This distinction is now specifically recognised in the rhinology literature. Alobid and colleagues have described self-induced nasal septal perforation from rhinotillexomania as a different entity from ordinary nose picking, with management that may require behavioural therapy, multidisciplinary care, silicone sheets, and septal repair where appropriate.[3]
For clinicians, the key question is not whether the behaviour is embarrassing. The key question is whether it is affecting healing.
Why the old “dry airflow” explanation is incomplete
Drying from nasal airflow is real. It is particularly relevant in patients with:
- a dry anterior septum
- exposed cartilage or bone
- postoperative crusting
- a septal perforation
- inflammatory nasal disease
- prior intranasal drug exposure
- mucosal injury from sprays, trauma, infection or surgery
But if airflow were the only driver, the clinical patterns would often be more predictable. What we commonly see is more focal and more mechanical.
The anterior septum is exactly where the finger reaches most easily. It is also where small areas of trauma can become chronic. A patient feels a dry crust or sharp edge, removes it, and creates a raw area. The raw area bleeds or weeps, then dries into another crust. The patient again feels blocked and clears it.
This is the crust–pick–crust cycle.
and excerpt from: Alobid I, Garaycochea O, Rojas-Lechuga MJ, Harvey RJ, Hopkins C, et al. International Consensus Statement on Nasal Septal Perforation. Rhinology. In press.
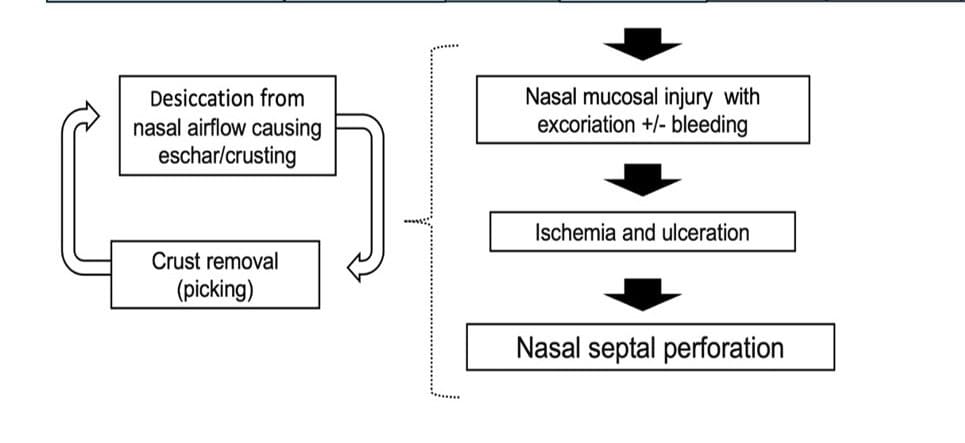
The recent International Consensus Statement on Nasal Septal Perforation supports this model. It describes a pathophysiological sequence from mucosal excoriation to ischaemia, ulceration and perforation. During that process, crust and eschar formation occur, and repeated removal of those crusts can further disrupt mucosal healing.[4] In the associated Delphi process, consensus was reached that nose picking driven by nasal crusting can be a factor in the pathogenesis of nasal septal perforation, and that nose picking can contribute to enlargement of an existing perforation.[4]
That is a major shift in thinking. Dryness may start the crust. The finger may stop it healing.
Scenario 1: chronic septal crusting without a perforation
The first clinical situation is the patient with chronic anterior septal crusting, but no established septal perforation.
These patients often say something like:
“I know I shouldn’t touch it, but I can feel something there. It blocks the airway. I just need to clear it.”
That statement is clinically important. The patient is not describing an irrational act. They are describing a sensory trigger. The crust feels obstructive, rough, dry, bloody or irritating. Removing it gives short-term relief. The long-term effect is the opposite: the area fails to heal.
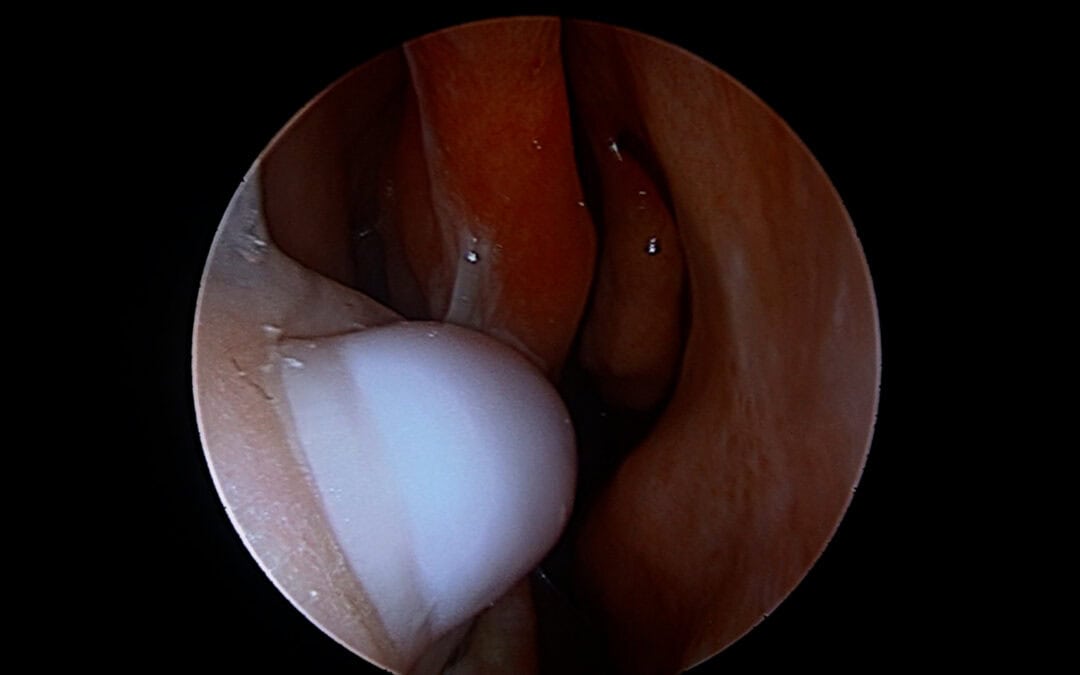
On endoscopy, the surgeon may see:
- focal anterior septal crusting
- a raw mucosal patch beneath the crust
- bleeding after crust removal
- squamous metaplasia or thickened unhealthy mucosa
- early ulceration over septal cartilage
- repeated crusting at the same reachable location
Persisent finger trauma results in the focal area of septal crusting
In selected patients, this becomes more than a moisturising problem. If the surface has become chronically unstable, it may need a reconstructive solution. A small mucosal graft can help restore a healthier epithelial surface and allow the area to re-mucosalise.
a simple free graft to the seputm can be used at any stage of the crusting to perforation stage to help with healing
The rationale is consistent with broader endoscopic rhinology experience. Free mucosal grafting has been used to accelerate re-epithelialisation, reduce crusting and stabilise healing surfaces in skull base surgery, frontal sinus surgery and septal reconstruction.[5] The aim is not simply to “cover a sore spot”. The aim is to interrupt the cycle of crusting, finger trauma and delayed healing.
Scenario 2: the already perforated septum
Septal perforations are often explained as airflow problems. That is partly correct. A hole in the septum changes airflow. Air moves abnormally through the perforation, secretions dry, and crusts form. Patients may develop obstruction, whistling, bleeding, crusting and impaired quality of life.
But the perforation itself also creates a target.
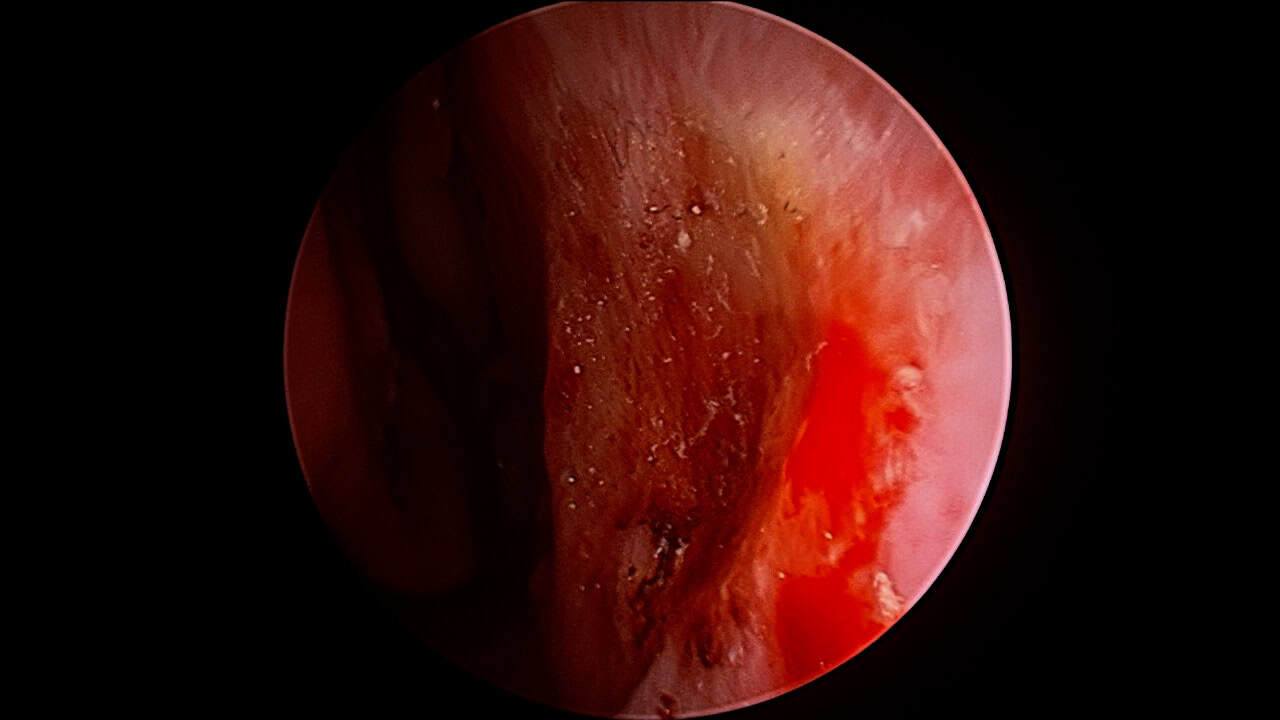
One of the most revealing clinical observations is crusting at the posterior edge of a septal perforation. Traditionally, that crusting might be explained by abnormal airflow across the back edge of the defect. In some cases, that is true. But it is not always the dominant factor.
Endoscopic video can show the finger entering the nose and picking directly at the posterior edge of the perforation. That image changes the explanation. The crust is not simply forming because air has passed over it. It is also being mechanically disturbed because the patient is trying to clear the obstruction.
This matters because ongoing picking can:
- enlarge the perforation
- maintain crusting at the perforation margin
- trigger recurrent bleeding
- prevent epithelial stability
- compromise the success of repair
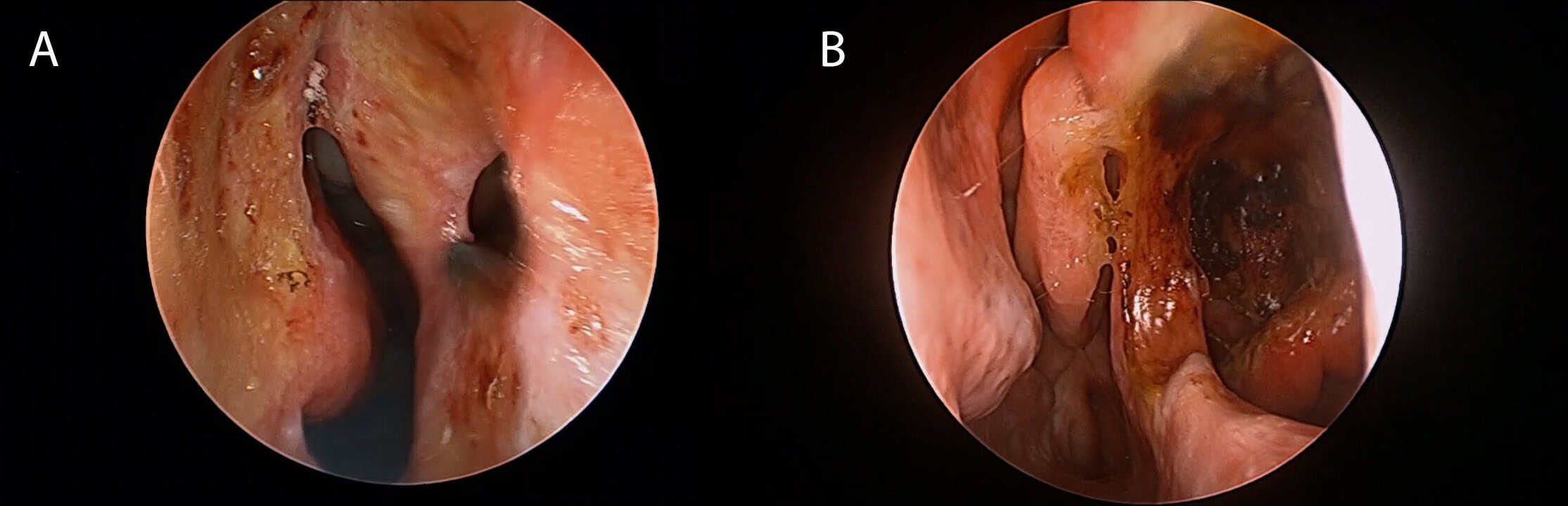
The areas of finger trauma are obvious in these patients with septal perforations.
Our own septal perforation repair cohort reflects how common this issue is in clinical practice. In a 90-patient series, picking was documented as present in 34.4% of patients, and picking was recorded as an aetiological factor in 22.2%. Most perforations were anterior, with 88.6% located anteriorly.[5]
Those numbers are not trivial. They suggest that nose picking is not an occasional incidental detail. It is a recurring clinical factor.
The same cohort also shows why restoring a stable mucosal surface matters. Before repair, crusting was present in 74.1% of patients. After repair, crusting fell to 12.9%. Ulceration fell from 14.0% to 2.3%, and anatomical closure was achieved in 90.0% of patients.[5] Free mucosal graft integration was complete in 85.6% overall, and complete in 92.6% of patients who achieved successful anatomical closure.[5]
These data support a practical point: if the mucosa is restored and protected, crusting and ulceration often improve substantially. But if the crust–pick–crust cycle continues, even technically sound repair may be placed at risk.
This is especially relevant when discussing perforations related to cocaine or other intranasal injury. The initiating factor may be chemical, vascular, traumatic or inflammatory. But the later non-healing phase often includes crusting, awareness, manipulation and repeated mucosal trauma.
Scenario 3: early septal trauma after septoplasty
The third situation is early septal trauma after an otherwise well-performed septoplasty.
Historically, when surgeons saw an early anterior septal ulcer or developing perforation after septoplasty, the explanation was often “poor blood supply”. Sometimes vascular compromise can occur. But that explanation does not always make anatomical sense.
The anterior septum has a rich blood supply. For matching injuries to occur on both sides of the septum, at the same anterior reachable location, purely from isolated vascular failure would be unusual. A more plausible explanation in many patients is early mechanical trauma.
After septoplasty, patients may feel:
- dried blood
- crusts
- sutures
- splints
- thick mucus
- obstruction
- sharp or rough edges
- anxiety that something is “stuck” in the nose
The natural reaction is to clear it. Unfortunately, the early postoperative septum is vulnerable. Fingertip trauma can remove healing mucosa, expose cartilage, and create bilateral opposing raw areas. If this is not recognised, a small area of trauma may progress to ulceration and then perforation.
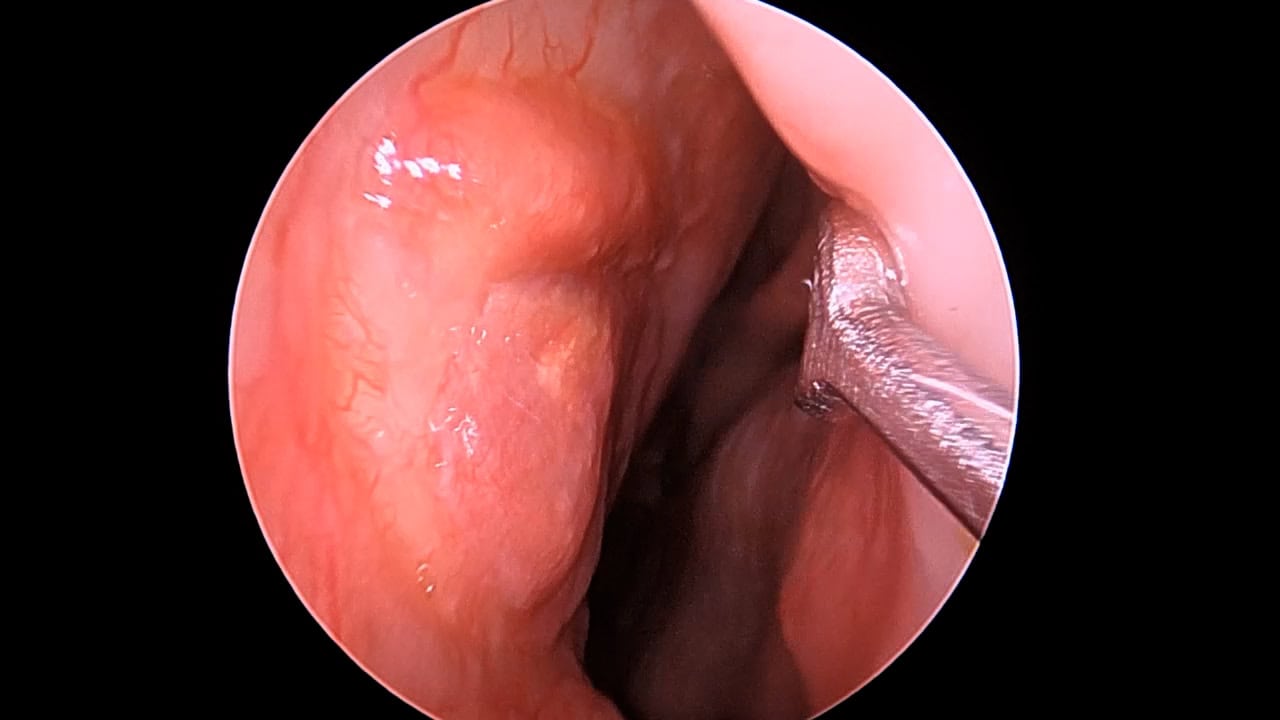
The practical observation is that these areas often heal very well when protected. Silastic sheets can shield the mucosa, reduce shear, maintain a moist environment and prevent direct finger trauma. In selected cases, mucosal grafting can also help restore the epithelial surface and get the healing process back on track.
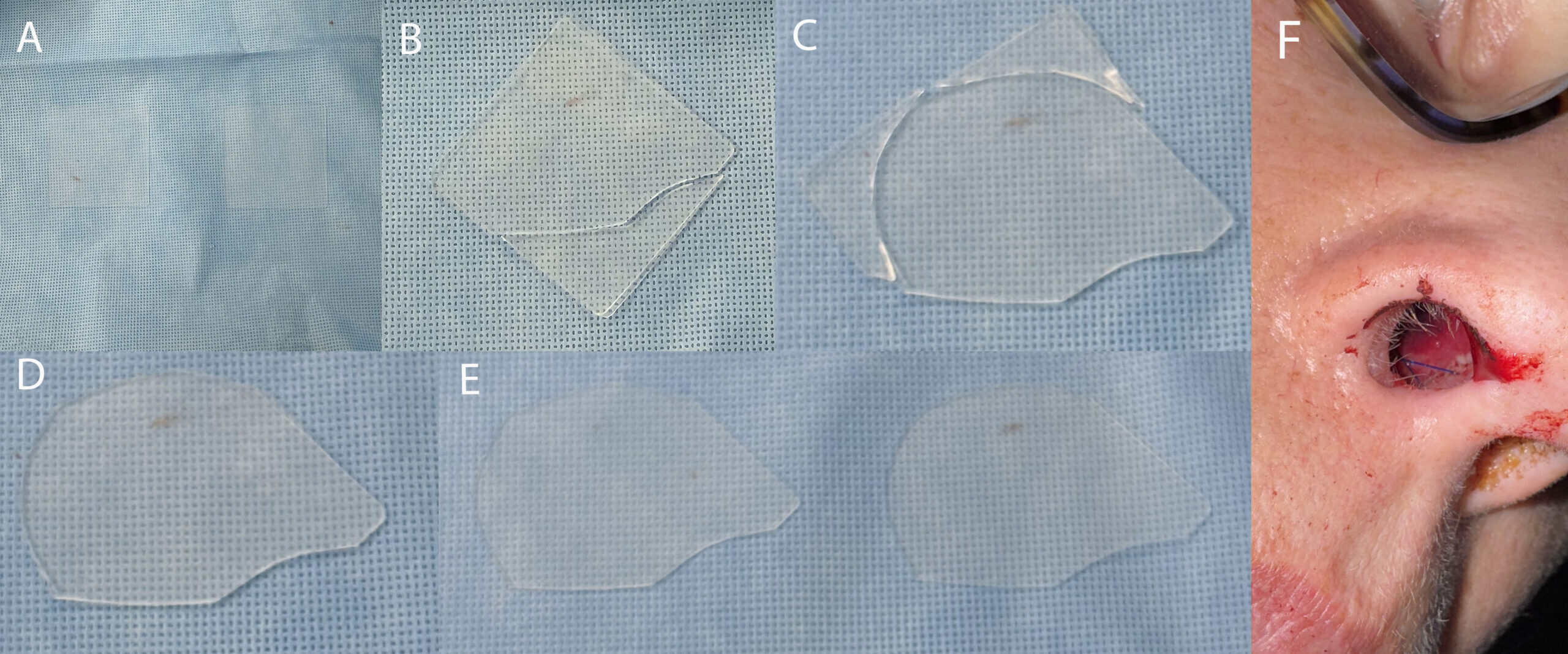
Simple silastic or silicone sheets are very helpful to ensure good healing and always best considered before crusting occurs
That response undermines the simplistic idea that the problem is always poor blood supply. If the tissue heals when protected from trauma and desiccation, then the issue was not simply irreversible vascular failure.
How to talk about this with patients
The conversation has to be direct, but not judgemental. Shame makes patients deny the behaviour. Denial prevents treatment.
A useful phrase is:
“I can see why you are clearing it. It feels blocked and uncomfortable. The problem is that every time the crust is removed with a finger, the healing surface is pulled off again. Our goal is not just to moisturise the nose. It is to stop the wound being reset every day.”
That explanation works because it validates the patient’s experience. The patient is not being accused of causing everything. They are being shown how one understandable behaviour can prevent healing.
Treatment usually involves several layers:
- saline irrigation or spray to soften crusts
- ointment or moisturising gel to reduce dryness
- avoidance of direct finger trauma
- careful debridement only when appropriate
- treatment of infection or inflammation if present
- protection with silastic sheets in selected cases
- mucosal grafting for focal non-healing areas
- septal perforation repair when the underlying drivers are controlled
- behavioural or psychological support when picking is compulsive
For true rhinotillexomania, the issue is not solved by telling the patient to “just stop”. Compulsive picking may sit within the broader group of body-focused repetitive behaviours and may require structured behavioural therapy, habit-reversal strategies and sometimes mental health support.[3]
A message for surgeons
Surgeons need to ask about nose picking. Not aggressively. Not sarcastically. Just plainly.
In septal crusting, septal ulceration, septal perforation and early postoperative septal trauma, the question is clinically relevant. If the behaviour is not recognised, the surgeon may keep treating the crust while missing the mechanism that recreates it.
This is now part of the modern septal perforation conversation. At Prof Isam Alobid’s International Septal Perforation Repair Course in Barcelona, where many of the major contemporary flap techniques are discussed, the role of crusting, mucosal injury and patient behaviour has become an important part of the discussion. I have jokingly been called the “nose picking expert” in this setting. It is not the most glamorous title in rhinology, but it is clinically useful.

Happy to known as the “Nose picking” expert, its a big part of clinical presentations.
The point is simple: good surgery still needs good healing conditions. If finger trauma continues, even technically excellent surgery may fail. If the behaviour is recognised and managed, many areas of septal crusting, ulceration and early trauma can recover.
Conclusion
Nose picking is common. Most of the time, it is harmless. But in the wrong clinical setting, it becomes important.
Chronic septal crusting, posterior-edge crusting in septal perforations, and early septal trauma after septoplasty are not always explained by airflow and dryness alone. The finger may be the missing mechanical factor.
The best approach is not blame. It is recognition. Patients pick because something feels blocked, dry, sharp or irritating. The surgeon’s job is to explain the crust–pick–crust cycle, reduce the crusting, protect the healing surface, and use reconstructive techniques such as silastic sheeting or mucosal grafting when needed.
Dry air may start the crust. The finger may stop it healing.
References
- Jefferson JW, Thompson TD. Rhinotillexomania: psychiatric disorder or habit? J Clin Psychiatry. 1995;56(2):56–59.
- Andrade C, Srihari BS. A preliminary survey of rhinotillexomania in an adolescent sample. J Clin Psychiatry. 2001;62(6):426–431.
- Alobid I, Arango Cabezas N, Yuen-Ato KC, Hopkins C, et al. Self-induced nasal septal perforation: rhinotillexomania — a different entity from nose picking. Laryngoscope. 2025;135(5):1590–1597. doi:10.1002/lary.31913.
- Alobid I, Garaycochea O, Rojas-Lechuga MJ, Harvey RJ, Hopkins C, et al. International Consensus Statement on Nasal Septal Perforation. Rhinology. In press.
- Campion NJ, Couto AM, Hua R, Qiao J, Gendeh H, Rosenbaum A, Darbari Kaul R, Alvarado R, Choy C, Sacks PL, Campbell RG, Kalish L, Harvey RJ. Free mucosal grafting as a simple adjunct to achieve rapid re-epithelialization in septal perforation repair. Laryngoscope. In press.
- Downs BW, Sauder HM. Septal Perforation. In: StatPearls. Treasure Island, FL: StatPearls Publishing; updated 2023.
FAQ
Is nose picking normal?
Yes. Nose picking is common and usually harmless. It becomes medically important when repeated picking damages vulnerable nasal lining, causes bleeding, worsens crusting, or prevents a septal wound from healing.
Can nose picking cause a septal perforation?
Nose picking can contribute to septal ulceration and perforation, especially when it repeatedly injures the same area of the anterior septum. It is rarely the only factor. Surgery, intranasal drugs, inflammation, infection, trauma and sprays may also contribute.
Why does septal crusting keep coming back?
Septal crusting can recur because of dryness, abnormal airflow, inflammation, exposed cartilage, infection or repeated mechanical trauma. In some patients, removing the crust with a finger repeatedly resets the wound surface and prevents stable healing.
Why does the back edge of a septal perforation crust?
The back edge of a septal perforation may crust because airflow through the perforation dries mucus. In some patients, however, the posterior edge is also repeatedly reached and traumatised by a finger when the patient tries to clear the crust.
Can picking after septoplasty cause problems?
Yes. Early after septoplasty, the nasal lining is healing and may be vulnerable. Picking at crusts, dried blood or sutures can injure the mucosa and, in some cases, contribute to septal ulceration or perforation.
How can septal crusting be treated?
Treatment usually includes saline sprays or irrigations, moisturising ointment or gel, treatment of infection or inflammation, and avoidance of direct trauma. In selected cases, silastic sheets or mucosal grafting may help protect and restore the healing surface.
What is rhinotillexomania?
Rhinotillexomania is compulsive, repetitive nose picking that may be difficult to control and can cause tissue injury. It is different from occasional ordinary nose picking and may require behavioural or psychological support.
“`html
“`