When the nose feels blocked but the airway is open: functional nasal obstruction and low-value nasal surgery
A common referral in tertiary rhinology is the patient who says: “I am a mouth breather,” “I never get enough oxygen,” or “my nose is ruining my sleep and energy.” Sometimes that patient has obvious nasal obstruction: a severe septal deviation, enlarged inferior turbinates, nasal polyps, allergic rhinitis or nasal valve collapse. In that setting, treatment can be high value.
But sometimes the nasal airway is already open.
The examination is unremarkable. The nose looks patent on endoscopy. Objective airflow testing is normal or near normal. The patient’s main concern is not really a blocked nostril, but fatigue, poor sleep, low energy, breathlessness, anxiety about breathing, or a general sense of not getting enough air.
That is a different clinical problem.
The nose filters, warms, humidifies and senses airflow. It is important for comfort, smell, airway protection and perceived sleep quality. But the nose does not oxygenate the blood. Gas exchange occurs in the lungs. Widening an already adequate nasal airway is unlikely to fix tiredness, poor energy, unexplained breathlessness or the feeling of “not getting enough oxygen.”
This is where Ray’s Rules become useful.
The turbinates are dynamic, not fixed
The inferior turbinates are vascular organs. They are not simply “large” or “small.” Their size changes through the day depending on posture, autonomic tone, allergy, rhinitis, irritants, infection, medication use and the normal nasal cycle.
Two normal physiological processes are especially important.
The first is the nasal cycle. This is the spontaneous alternating congestion and decongestion of the nasal mucosa. One side of the nose becomes more congested while the other side opens. This is driven by dilation and constriction of venous cavernous tissue in the turbinates and septum. Approximately 70–80% of healthy adults demonstrate a nasal cycle, although the pattern is not always perfectly regular or symmetrical. The cycle length may vary from 30 minutes to several hours.¹
The second is postural congestion. When a person moves from sitting upright to lying flat, central venous pressure may increase by up to approximately 8 mmHg because of hydrostatic pressure. This increases congestion of the nasal mucosa and nasal airway resistance. The effect is often greater when lying on one side, where the lower, dependent nasal cavity becomes more congested.¹,²
These normal physiological changes are amplified when the nasal lining is already inflamed or vascularly reactive, as occurs in allergic rhinitis, non-allergic rhinitis and inferior turbinate hypertrophy.
This explains why patients with true turbinate-driven obstruction often say:
“It swaps sides.”
“It is worse when I lie down.”
“It blocks on the side I sleep on.”
“A decongestant spray opens it clearly.”
That history is not incidental. It is diagnostic information.
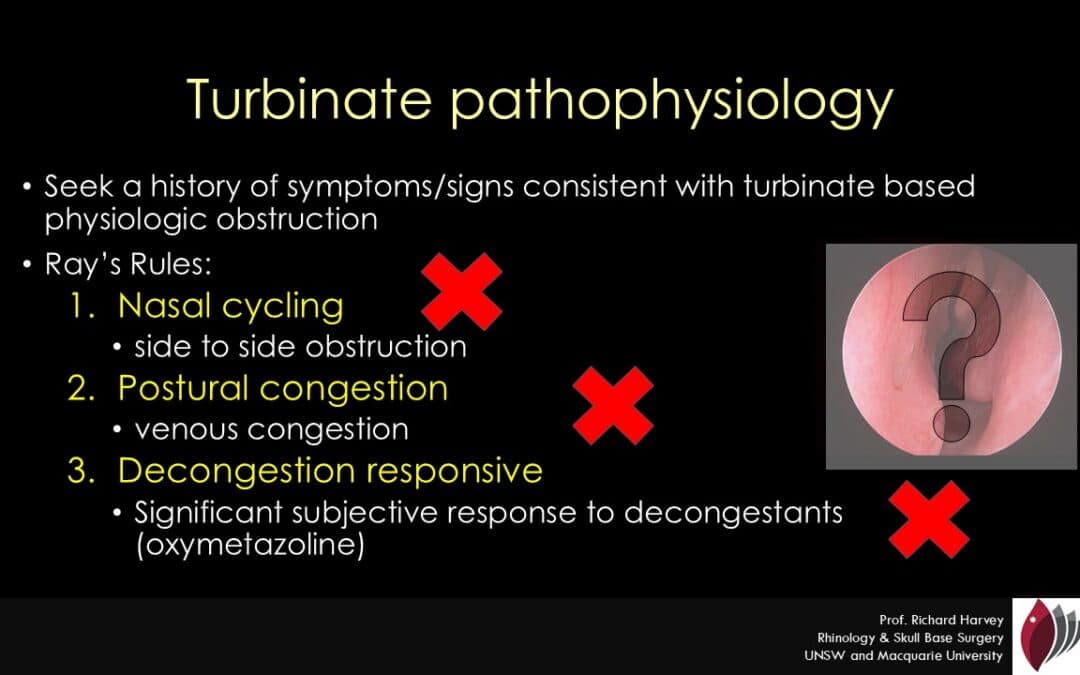
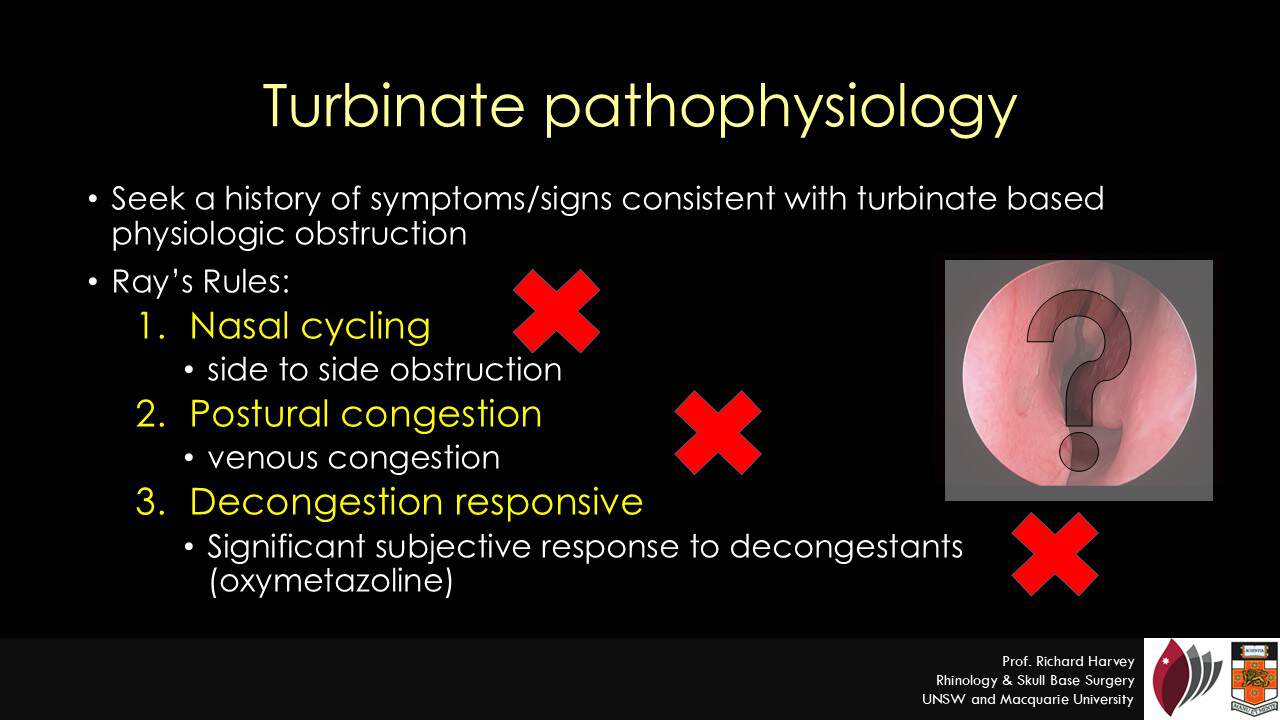
Ray’s Rules: a practical test of turbinate physiology
Ray’s Rules are a simple clinical heuristic for deciding whether a patient’s symptoms behave like vascular turbinate obstruction.
They ask whether the patient has:
- Cycling nasal congestion — the blocked side changes from side to side.
- Postural congestion — the nose blocks when lying flat or on the dependent side.
- A clear response to topical decongestant — the airway improves when the vascular turbinate component is temporarily reduced.
These features suggest that the patient has an intact sensory perception of nasal airflow and a dynamic turbinate component to their obstruction. In other words, the symptoms behave like turbinate disease.³,⁴
This does not mean that every patient with positive Ray’s Rules needs surgery. Many still need medical management first: saline irrigation, intranasal corticosteroids, antihistamines, allergen avoidance, immunotherapy where appropriate, and treatment of rhinitis. But if symptoms persist despite well-conducted medical therapy, and the examination confirms inferior turbinate hypertrophy, turbinate reduction may be a rational intervention.
The important point is the reverse: patients who do not demonstrate these features may be poor candidates for turbinate surgery, particularly when objective findings are mild.
Ray’s rules provide a simple pathophysioology linked screen for patients likely to benefit from turbinate reduction
When nasal surgery is more likely to be high value
Nasal surgery is more likely to be high value when there is a match between the patient’s symptoms, examination and objective findings.
For example, a patient with visible inferior turbinate hypertrophy, alternating nasal obstruction, night-time postural blockage and a strong response to decongestant has a plausible vascular turbinate problem. If medical treatment fails, turbinate reduction may address the mechanism of obstruction.
Similarly, a patient with a clear anterior septal deviation, nasal valve compromise, or fixed unilateral obstruction has a structural problem that may be improved by septoplasty, septorhinoplasty or valve surgery.
In both settings, the treatment target is clear: improve nasal airflow through a mechanically or physiologically obstructed nasal airway.
When nasal surgery may be low value
Surgery becomes low value when the patient’s main symptoms are not actually explained by the nose.
A common example is the patient who presents with “nasal congestion” but, on closer questioning, is primarily concerned about:
- poor sleep
- waking unrefreshed
- fatigue
- low daytime energy
- reduced exercise tolerance
- breathlessness
- feeling they are “not getting enough oxygen”
- anxiety around breathing
- a general belief that mouth breathing is damaging their health
Many of these patients have become more aware of nasal breathing through popular health culture. Books such as James Nestor’s Breath: The New Science of a Lost Art have brought attention to nasal breathing, slow breathing, mouth breathing, breathwork and the relationship between breathing habits and health.⁵ This public discussion has been useful in many respects. Nasal breathing is physiologically preferable to chronic mouth breathing. It filters and humidifies air, supports nasal airflow sensation, and contributes to airway comfort.
But the popular message can become distorted. Some patients begin to attribute almost every symptom — fatigue, poor sleep, reduced concentration, exercise limitation, anxiety or “low oxygen” — to minor nasal findings. That is not good medicine.
If the nasal airway is open, airflow testing is normal, and the patient does not describe cycling congestion, postural congestion or decongestant response, then turbinate surgery is unlikely to solve the true problem. In that situation, it is more useful to look for other contributors: sleep apnoea, insomnia, stress, anxiety, poor sleep routine, medication effects, cardiopulmonary disease, anaemia, endocrine issues, deconditioning or broader health factors.
Telling the patient that nasal surgery is not indicated is not dismissive. It may be the most honest and protective answer.
Nasal breathing and sleep: important, but not magic
There is good evidence that treating nasal disease can improve subjective sleep quality. A systematic review and meta-analysis of allergic rhinitis and nasal septal deviation found that treatment improved patient-reported sleep measures, including Epworth Sleepiness Scale and Pittsburgh Sleep Quality Index scores.⁶
However, the same review found insufficient evidence that objective sleep metrics improve in the same way.⁶ This distinction matters.
A patient may feel that sleep is better after nasal treatment. That is a valid outcome. Better nasal airflow can reduce discomfort, reduce mouth breathing, improve CPAP tolerance in selected patients, and improve sleep-related quality of life. But improvement in nasal airflow sensation is not the same as better sleep function.
But nasal surgery should not be presented as a reliable treatment for objective sleep architecture, oxygenation, sleep apnoea or global fatigue unless the broader sleep disorder has been properly assessed. The nose contributes to sleep comfort. It is not the whole sleep system.
Functional nasal obstruction and unrealistic expectations
The most difficult group is the patient with severe symptoms, minimal objective obstruction and high expectations of benefit from surgery.
Some patients describe nasal obstruction in a way that resembles breathlessness, air hunger or anxiety about breathing. In the empty nose syndrome and functional nasal obstruction literature, this mismatch between symptoms and objective findings has become increasingly important. Patients may present before surgery with nasal airflow symptoms that are not explained by anatomy, then remain symptomatic or worsen after a technically adequate septal or turbinate procedure.³,⁴
This does not mean the symptoms are fake. It means the mechanism may not be surgically correctable.
In this setting, further surgery can be harmful. It may reinforce the belief that the problem is purely structural, create disappointment when the expected gains in sleep or energy do not occur, and expose the patient to the risks of an operation without a realistic chance of solving the primary complaint.
Ray’s Rules help identify the patient whose symptoms behave like turbinate physiology. They also help identify the patient in whom turbinate surgery may be the wrong tool. A terrific summary article by Professor Sacks is availiable here.
Why the profession needs to own this problem
Functional nasal surgery is under increasing scrutiny. In 2025, ENT UK expressed concern about South-East England ICB decisions to suspend funding for septoplasty, turbinate surgery and functional septorhinoplasty.⁷ Media coverage reported that some patients would receive NHS septoplasty funding only in exceptional circumstances.⁸
Blunt funding restrictions are not the right way to manage nasal obstruction. Some patients have severe, genuine, surgically correctable nasal airway disease. They need access to high-value nasal surgery.
But the profession also needs to be clear about where surgery is less likely to help. If surgeons do not define high-value nasal surgery carefully, funders may define it crudely.
A simple heuristic of “failed nasal steroid spray, therefore septoplasty and turbinate reduction” is not enough. Good decision-making should include the patient’s symptom pattern, endoscopy, objective airflow assessment where appropriate, response to decongestant, allergy/rhinitis evaluation and the patient’s expectations of benefit.
The practical message
Ray’s Rules are not a formal score. They are a practical clinical safeguard.
If the nose blocks from side to side, worsens with posture, and opens with decongestant, the symptoms are behaving like turbinate physiology. If examination confirms turbinate hypertrophy and medical therapy has failed, turbinate surgery may be a reasonable high-value intervention.
If the patient’s main concern is sleep, fatigue, tiredness, breathlessness or not getting enough oxygen, and the nasal airway is objectively adequate, nasal surgery is unlikely to solve the real problem.
A good rhinologist does not just widen noses. A good rhinologist decides when widening the nose is likely to help — and when it is not.
References
- Pendolino AL, Lund VJ, Nardello E, Ottaviano G. The nasal cycle: a comprehensive review. Rhinology Online. 2018;1:67–76. doi:10.4193/RHINOL/18.021.
- Harvey RJ, Roland LT, Schlosser RJ, Pfaar O. Chief Complaint: Nasal Congestion. J Allergy Clin Immunol Pract. 2024;12(6):1462–1471. doi:10.1016/j.jaip.2024.04.028.
- Kanjanawasee D, Campbell RG, Rimmer J, Alvarado R, Kanjanaumporn J, Snidvongs K, Kalish L, Harvey RJ, Sacks R. Empty nose syndrome pathophysiology: a systematic review. Otolaryngol Head Neck Surg. 2022;167(3):434–451. doi:10.1177/01945998211052919.
- Png LH, Kalish L, Sacks R. Empty nose syndrome: the case for “functional nasal obstruction” as a predisposing risk prior to nasal surgery. Curr Otorhinolaryngol Rep. 2023;11:422–429. doi:10.1007/s40136-023-00487-w.
- Nestor J. Breath: The New Science of a Lost Art. New York: Riverhead Books; 2020.
- Fried J, Yuen E, Zhang K, Li A, Rowan NR, Schlosser RJ, Nguyen SA, Gudis DA. Impact of treatment for nasal cavity disorders on sleep quality: systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2022;166(4):633–642. doi:10.1177/01945998211029527.
- ENT UK. Statement concerning the suspension of funding for functional nasal surgery. Published 10 October 2025.
- Tapper J. NHS cuts will “severely impact” those who struggle to breathe. The Observer. Published 6 October 2025
FAQ
What is functional nasal obstruction?
Functional nasal obstruction describes a situation where a patient feels significantly blocked, but the nasal airway is open or near normal on examination and objective testing. The symptom is real, but the mechanism may not be a surgically correctable narrowing of the nose.
What are Ray’s Rules?
Ray’s Rules are a practical rhinology heuristic used to identify whether symptoms behave like turbinate-driven obstruction. The three features are cycling nasal congestion, postural congestion and a clear response to topical nasal decongestant.
What is cycling nasal congestion?
Cycling nasal congestion means the blocked side changes from one side of the nose to the other. This often reflects the normal nasal cycle, where one side of the nose becomes more congested while the other side opens.
What is postural nasal congestion?
Postural nasal congestion is nasal blockage that worsens when lying flat or lying on one side. It occurs because venous pressure and vascular congestion increase in the nasal lining, especially around the inferior turbinates.
Does a blocked nose cause low oxygen levels?
Usually no. The nose filters, warms, humidifies and senses airflow, but gas exchange occurs in the lungs. A blocked nose can affect comfort, perceived sleep quality and mouth breathing, but persistent breathlessness or concern about oxygen levels should be assessed beyond the nose.
Can nasal surgery improve sleep?
Nasal surgery and rhinitis treatment can improve patient-reported sleep quality in selected patients. However, evidence that nasal surgery reliably improves objective sleep measurements, sleep architecture or oxygenation is limited.
When is turbinate surgery more likely to help?
Turbinate surgery is more likely to help when symptoms behave like turbinate physiology: the blockage cycles from side to side, worsens with posture, improves with decongestant, and examination confirms inferior turbinate hypertrophy.
When is nasal surgery less likely to help?
Nasal surgery is less likely to help when the nasal airway is already open, airflow testing is normal, and the main concerns are fatigue, poor energy, breathlessness, poor sleep or a general feeling of not getting enough oxygen.