Why Immunotherapy Should Not Be the Last Step in Allergic Rhinitis
Allergic rhinitis is often treated as a symptom problem. A patient has sneezing, runny nose, itching, watery eyes or nasal congestion, so treatment is aimed at suppressing those symptoms. Intranasal corticosteroid sprays, antihistamines and leukotriene receptor antagonists can all be useful. For short-lived allergy, such as a few weeks of seasonal pollen symptoms, this approach is entirely reasonable.
The problem is different when the allergy is chronic.
House dust mite allergy is not a two-week problem. For many patients, it is a decade-long or lifelong inflammatory exposure. In that setting, simply suppressing the allergic response year after year with pharmacotherapy is not always a long-sighted strategy. It may control symptoms, but it does not meaningfully change the allergic disease process.
This is where allergen immunotherapy deserves a different place in the treatment discussion.
Pharmacotherapy suppresses symptoms; immunotherapy modifies the disease
The conventional allergic rhinitis treatment ladder usually begins with pharmacotherapy. Patients are offered antihistamines, nasal steroid sprays, combination sprays or leukotriene antagonists. Immunotherapy is often considered later, when symptoms are severe, when multiple organs are involved, or when the patient has failed standard medical treatment.
That sequence makes sense for some patients. It makes less sense for a teenager or young adult with clear house dust mite allergy, chronic nasal congestion and years of disease ahead.
The distinction is simple:
- Pharmacotherapy suppresses the allergic response while it is being used.
- Allergen immunotherapy aims to change the immune response to the allergen.
This does not mean immunotherapy is needed for every patient with allergic rhinitis. It does mean that for persistent house dust mite allergy, especially when nasal obstruction is chronic, immunotherapy should be discussed much earlier than it often is.
The question should not simply be, “Can we suppress the symptoms?” The better question is, “What is the long-term plan for this allergic disease?”
Why house dust mite allergy is different
Seasonal allergic rhinitis can be episodic. A patient may have symptoms for a few weeks or months, then recover for the rest of the year. In that setting, using medication during the season is practical.
House dust mite allergy is usually perennial. The exposure occurs in the bedroom, mattress, carpet, clothing and indoor environment. The patient is not simply reacting to an occasional allergen. They are living with a persistent allergic stimulus.
That matters clinically because persistent allergic inflammation can produce more than sneezing and a runny nose. It can contribute to chronic nasal congestion — and nasal congestion is not always the same as nasal obstruction — turbinate swelling, middle turbinate oedema, sleep disturbance, mouth breathing and reduced quality of life..
A treatment strategy based only on symptom suppression may be too passive for that type of patient.
The evidence base for immunotherapy is not small
One reason immunotherapy is still under-discussed is that it is sometimes treated as a niche or late-stage option. That is difficult to justify from the evidence base.
A recent network meta-analysis by Zhang and colleagues compared biologics, allergen immunotherapy and pharmacotherapies for moderate-to-severe allergic rhinitis.[1] The analysis included 28 randomised controlled trials involving 13,312 participants. It compared biologics, allergen immunotherapy and key pharmacotherapies, including intranasal corticosteroids alone or in combination with antihistamines.
For short-term nasal symptom control, biologics performed best. Anti-IL-4Rα therapy ranked highest for Total Nasal Symptom Score, followed by anti-IgE therapy. Allergen immunotherapy ranked below biologics but above all pharmacotherapies for nasal symptom control.[1]

Foreest plots of comparative efficacy and safety for all interventions versus placebo in treating moderate-to-severe allergic rhinitis. (a) Mean difference in TNSS change from the baseline. (b) Mean difference in TOSS change from the baseline. (c) Mean difference in RQLQ change from the baseline. (d) Risk ratio in AE. CI, confidence interval; INAH, intranasal antihistamines; INCS, intranasal corticosteroids; OAH, oral antihistamines; RQLQ, Rhinitis Quality of Life Questionnaire; RR, risk ratio; TNSS, Total Nasal Symptom Score; TOSS, Total Ocular Symptom Score.
That result needs to be interpreted correctly.
Biologics are powerful targeted suppressive therapies. They may have a future role in severe, refractory or multi-system type 2 inflammatory disease. But for ordinary persistent allergic rhinitis, biologics are unlikely to become routine first-line treatment because of cost, access and the need for longer-term safety data in otherwise non-life-threatening allergic disease.
Allergen immunotherapy occupies a different position. It is not merely another suppressive treatment. It is the treatment class directed at modifying the allergic mechanism itself. In the Zhang analysis, even within a short-term comparison window, immunotherapy outperformed pharmacotherapy for nasal symptoms.[1] Its real value is likely greater than that short-term ranking suggests, because immunotherapy is intended to induce longer-term immune tolerance, not simply produce rapid symptom suppression.
The broader allergy literature also supports the idea that immunotherapy is not just a “nose treatment”. In a Cochrane review of injection immunotherapy for asthma, 88 randomised trials were included. There were 42 trials of house dust mite immunotherapy, 27 pollen trials, 10 animal dander trials and additional mould, latex and multi-allergen trials. Immunotherapy significantly reduced asthma symptoms and medication use and improved bronchial hyper-reactivity. The review estimated that only three patients needed treatment to avoid one deterioration in asthma symptoms, and four needed treatment to avoid one patient requiring increased medication.[2]
The skin literature is more cautious, but still relevant to the broader allergic disease discussion. A Cochrane review of specific allergen immunotherapy for atopic eczema identified 12 randomised controlled trials involving 733 participants, most involving house dust mite allergy. The evidence was lower quality and the results were less consistent than in allergic rhinitis and asthma. Some investigator-rated outcomes improved, but participant-reported eczema outcomes were less convincing.[3] This should not be overstated. Immunotherapy is not a universal solution for every atopic disease. But the existence of randomised trial evidence across rhinitis, asthma and eczema reinforces the larger point: immunotherapy is a serious disease-modifying strategy, not an alternative-health add-on.
This is why patient surprise is understandable. Many patients with persistent allergic rhinitis ask, “Why wasn’t this discussed with me earlier?” For a patient with confirmed house dust mite allergy, chronic symptoms and years of expected disease, that is a fair question.
Oral tablets have changed the practicality of immunotherapy
Historically, immunotherapy was often thought of as injection therapy. Subcutaneous immunotherapy is effective, but it requires repeated injections, clinic attendance and post-injection monitoring. It also carries a risk of systemic allergic reactions, including rare severe reactions.
Sublingual immunotherapy has changed the practical discussion. Modern house dust mite sublingual immunotherapy tablets or wafers use standardised allergen extracts and fixed dosing. They are placed under the tongue and are easier to initiate and continue than many older aqueous drop regimens.
A 2026 meta-analysis comparing subcutaneous immunotherapy and sublingual immunotherapy in allergic rhinitis included six randomised controlled trials and 588 participants.[4] It found no statistically significant difference in treatment discontinuation between subcutaneous and sublingual immunotherapy. However, adverse events were significantly higher with subcutaneous immunotherapy than with sublingual immunotherapy.[4]
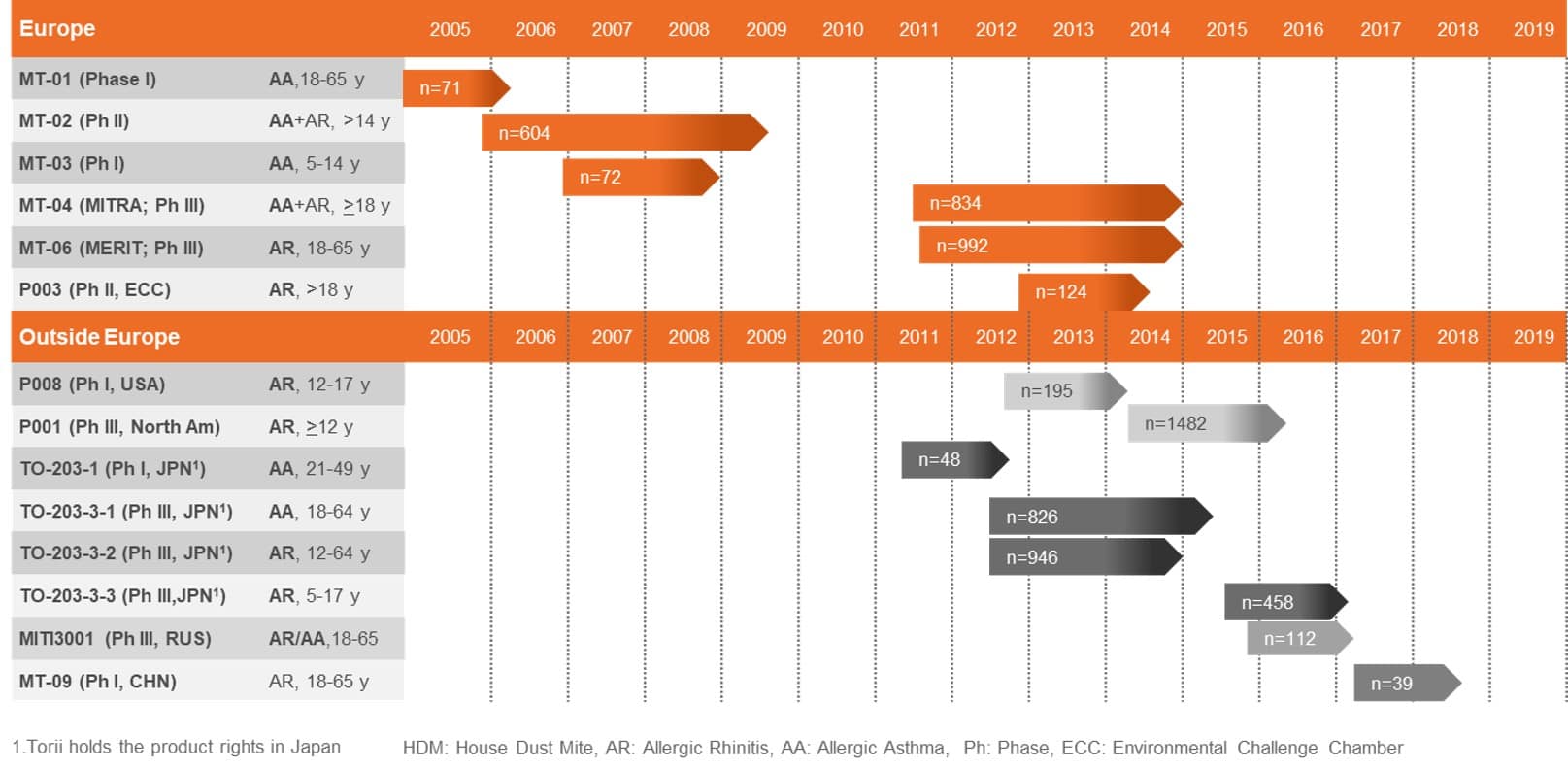
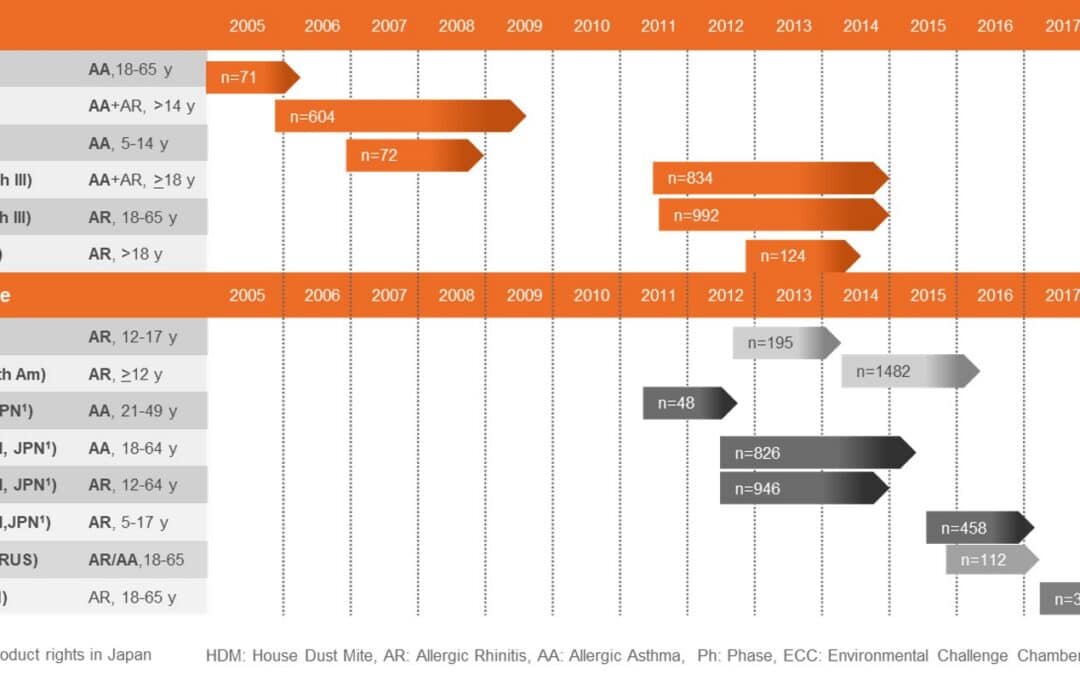
Evidence base for oral allergen immunotherapy in persistent allergic rhinitis, showing randomised controlled trials and systematic reviews supporting disease-modifying treatment.
This does not prove that sublingual immunotherapy is more effective. It does suggest that, when efficacy is broadly comparable and convenience and safety matter, sublingual tablet therapy is a very reasonable starting point for many patients.
That is particularly relevant in routine allergic rhinitis care. A teenager with chronic house dust mite allergic rhinitis is more likely to accept a daily sublingual wafer than repeated injection visits. If the goal is to start disease-modifying therapy early, the ease of use matters.
The patient journey is the missing part of the decision
The traditional question is:
“Are the symptoms bad enough to justify immunotherapy?”
That is the wrong question for many patients.
A better question is:
“Is this a chronic allergic disease that the patient is likely to manage for years or decades?”
For persistent house dust mite allergy, the answer is often yes. If a 15-year-old has chronic nasal congestion, proven house dust mite sensitisation, clear allergic findings on examination and ongoing symptoms, then simply prescribing years of sprays and antihistamines may not be the most strategic plan. This is also where clinicians need to separate allergic mucosal disease from functional nasal obstruction, because the treatment strategy should follow the mechanism rather than the symptom label.
A more useful treatment conversation is:
- What is the allergic driver?
- Is the allergen avoidable or persistent?
- Is the patient likely to need treatment for months, years or decades?
- Is the nose showing tissue effects of allergy, not just symptoms?
- Would disease modification be more sensible than repeated suppression?
- If pharmacotherapy is used, what is the review point and exit strategy?
The last question is particularly important. Patients should not drift for years on partly effective medication without a plan.
Central compartment atopic disease shows why this matters
Central compartment atopic disease, or CCAD, is a good example of the problem. CCAD is an allergic tissue-remodelling condition affecting the central part of the nose, including the middle turbinate, superior septum, superior turbinate and uncinate region.[5,6] It can be understood as part of a spectrum of inhalant allergy in which chronic exposure leads to visible mucosal change.
These patients often have house dust mite sensitisation. They may have nasal obstruction, pressure symptoms, smell disturbance, sinus symptoms and polypoid central compartment change. By the time they require surgery, pharmacotherapy has usually already failed to prevent progression.
That is why simply operating and then placing the patient back on the same pharmacotherapy that failed before surgery is conceptually weak.
Surgery can remove obstructing tissue and improve sinus ventilation. It can reduce the burden of polypoid remodelling. But surgery does not switch off the inhalant allergy that drove the disease in the first place.
In a retrospective cohort study of surgically treated, house dust mite-sensitised CCAD patients, 86 patients were assessed after surgery.[6] All patients receiving allergen immunotherapy had started it before surgery. At 12 months, patients treated with immunotherapy had significantly less recurrent middle turbinate oedema than those not receiving immunotherapy: 15.6% versus 52.9% with diffuse or worse oedema.[6] They also required less frequent topical corticosteroid irrigation: 37.5% versus 79.6% using corticosteroid irrigations four or more times per week.[6]
Symptoms were similar between the groups at 12 months, but the endoscopic and treatment-burden findings are the more important signal. Immunotherapy appeared to reduce allergic tissue activity and allowed de-escalation of pharmacotherapy.[6]
That is exactly the strategic point. If the disease process is allergic tissue remodelling, then postoperative care should not simply be more pharmacological suppression. It should include disease modification.
A more rational treatment strategy for persistent allergic rhinitis and CCAD
For persistent house dust mite allergic rhinitis, immunotherapy should sit at the centre of the long-term treatment strategy.
Pharmacotherapy still has a role, but that role should be understood clearly. Nasal steroid sprays, antihistamines and other suppressive treatments are useful for short-term symptom control, especially during flares. These flares are common with viral upper respiratory tract infections, seasonal exposure changes, dust exposure, sleep disruption or other inflammatory triggers.
But for chronic allergic disease, pharmacotherapy should not be the whole plan.
A more rational approach is:
- Confirm the allergic driver with history, examination and allergy testing.
- Assess the nose objectively, including endoscopy and objective nasal airflow and allergy testing when symptoms are persistent, obstructive or not responding as expected.
- Place allergen immunotherapy at the centre of the long-term strategy when house dust mite allergy is perennial and clinically relevant.
- Use pharmacotherapy for short-term disease suppression, exacerbations and bridging while immunotherapy takes effect.
- Consider sublingual tablet immunotherapy early for many patients because it is standardised, convenient and avoids the injection-related systemic reaction risk of subcutaneous therapy.
- Consider surgery only when there is structural obstruction, turbinate hypertrophy or tissue remodelling that will not reverse with allergy treatment alone. This is the same broader principle discussed in “septal deviation and big turbinates” is not a diagnosis: surgery helps when it addresses the correct mechanism, but it is not a substitute for diagnosing and treating the underlying inflammatory driver.
- After surgery for CCAD or allergic tissue remodelling, avoid returning the patient to the same failed pharmacotherapy-only strategy.
This is particularly relevant for teenagers and young adults. A chronic dust mite allergic nose at age 15 is not a short-term medication problem. It is a long-term airway management problem.
Why this should be discussed early
There is no good reason for a patient with persistent allergic rhinitis to learn about immunotherapy only after years of sprays, antihistamines and frustration.
The threshold for discussing immunotherapy should be low when:
- symptoms are perennial rather than seasonal
- house dust mite sensitisation is clear
- nasal congestion is chronic
- the patient is young and likely to live with the disease for decades
- there is asthma, eczema, conjunctivitis or broader atopic disease
- endoscopy shows allergic tissue effects such as middle turbinate oedema
- pharmacotherapy is needed continuously rather than intermittently
- surgery is being considered for allergic tissue remodelling
Discussing immunotherapy is not the same as forcing it on every patient. It is giving the patient a proper long-term framework.
If immunotherapy has level 1 evidence in allergic rhinitis and asthma, if modern sublingual preparations are standardised and practical, and if persistent house dust mite allergy is a long-term disease, then immunotherapy should be raised early. It is hard to justify otherwise.
Conclusion
Allergic rhinitis should not always be treated as a short-term symptom disorder. For seasonal symptoms, pharmacotherapy is often sensible and sufficient. For persistent house dust mite allergy, the thinking should be different.
Pharmacotherapy suppresses symptoms. It has value during exacerbations, viral upper respiratory flares and short-term symptom deterioration. But it does not alter the allergic immune response in the same way as allergen immunotherapy.
The recent comparative evidence shows that allergen immunotherapy performs better than pharmacotherapy for nasal symptom control in moderate-to-severe allergic rhinitis, while biologics offer the strongest short-term suppression but are unlikely to be routine therapy for simple allergic rhinitis.[1] Cochrane data in asthma show a substantial randomised trial evidence base for immunotherapy improving symptoms, medication use and bronchial hyper-reactivity.[2] Direct comparison data in allergic rhinitis suggest sublingual immunotherapy has practical safety advantages over subcutaneous immunotherapy, with no clear disadvantage in treatment discontinuation.[4]
That matters most when the allergic burden is measured in decades, not weeks.
In patients with chronic house dust mite allergy, persistent congestion or allergic tissue remodelling, immunotherapy should not be reserved only for the end of the treatment pathway. It should be discussed early as part of a long-term strategy.
The goal should not be indefinite suppression of allergy. The goal should be to change the allergic trajectory.
References
- Zhang Z, Fang D, Wang C, Zhang Y, Zhang L. Efficacy and safety of biologics, allergen immunotherapy, and pharmacotherapies for moderate-to-severe allergic rhinitis: a network meta-analysis. Int Forum Allergy Rhinol. 2026;16:582–594. doi:10.1002/alr.70108.
- Abramson MJ, Puy RM, Weiner JM. Injection allergen immunotherapy for asthma. Cochrane Database Syst Rev. 2010;(8):CD001186. doi:10.1002/14651858.CD001186.pub2.
- Tam H, Calderon MA, Manikam L, Nankervis H, García Núñez I, Williams HC, Durham S, Boyle RJ. Specific allergen immunotherapy for the treatment of atopic eczema. Cochrane Database Syst Rev. 2016;(2):CD008774. doi:10.1002/14651858.CD008774.pub2.
- Wang D, Song D, Xu X. Efficacy of allergen-specific immunotherapy for allergic rhinitis: a meta-analysis. Front Med. 2026;13:1759079. doi:10.3389/fmed.2026.1759079.
- DelGaudio JM, Loftus PA, Hamizan AW, Harvey RJ, Wise SK. Central compartment atopic disease. Am J Rhinol Allergy. 2017;31(4). doi:10.2500/ajra.2017.31.4443.
- Meerwein CM, Sacks PL, Ho J, Choy C, Kalish L, Campbell RG, Sacks RR, Harvey RJ. The effect of allergen immunotherapy in patients with central compartment atopic disease post-surgery. Int Forum Allergy Rhinol. 2025;15:128–134. doi:10.1002/alr.23459.
- Hamizan AW, Christensen JM, Ebenzer J, Oakley G, Tattersall J, Sacks R, et al. Middle turbinate edema as a diagnostic marker of inhalant allergy. Int Forum Allergy Rhinol. 2017;7(1):37–42.
FAQ
Is house dust mite allergy a long-term condition?
Yes. House dust mite allergy is usually perennial, meaning exposure occurs throughout the year. For many patients it is a long-term allergic condition measured in years or decades rather than weeks.
What is allergen immunotherapy?
Allergen immunotherapy is a treatment that exposes the immune system to controlled doses of an allergen, such as house dust mite, with the aim of reducing allergic sensitivity over time. It is often called desensitisation.
How is immunotherapy different from nasal sprays or antihistamines?
Nasal sprays and antihistamines suppress allergic symptoms while they are being used. Immunotherapy aims to modify the immune response to the allergen itself, which is why it is considered a disease-modifying treatment.
Should immunotherapy be discussed early for allergic rhinitis?
Yes. Immunotherapy should be discussed early when allergic rhinitis is persistent, clinically relevant and likely to require treatment for many years. Discussing immunotherapy does not mean every patient must start it, but patients should understand the long-term option.
Is sublingual immunotherapy as effective as injection immunotherapy?
Evidence suggests that sublingual and subcutaneous immunotherapy can both be effective. Direct comparison studies have not shown a major difference in treatment discontinuation, while adverse events are generally higher with injection immunotherapy.
Why might oral immunotherapy tablets be useful?
Modern sublingual tablets or wafers use standardised allergen extracts and fixed dosing. They are convenient, avoid repeated injection visits and are often easier for patients to accept as a long-term treatment.
What is central compartment atopic disease?
Central compartment atopic disease, or CCAD, is an allergic tissue-remodelling condition affecting the central part of the nose, including the middle turbinate, superior septum and nearby structures. It is commonly associated with inhalant allergy, including house dust mite allergy.
Does surgery treat the allergy in CCAD?
No. Surgery may improve obstruction, remove polypoid tissue and improve sinus ventilation, but it does not switch off the underlying inhalant allergy. That is why allergen immunotherapy may be important after surgery in selected patients.