The word polyp sounds precise. In many parts of medicine, it implies a discrete growth that needs to be identified, biopsied, removed or monitored. In the nose, however, the word is much less precise.
A nasal polyp is often not a diagnosis. It is usually an examination finding.
That distinction matters because very different diseases can produce polypoid tissue inside the nose. Some polyps are part of a diffuse inflammatory airway disorder. Some are related to simple inhalant allergy. Some are benign proliferative lesions. Some arise in genetic conditions such as cystic fibrosis. Some are isolated anatomical lesions such as antrochoanal polyps. Radiology reports may even call a mucous retention cyst in a sinus a “polyp,” which adds another layer of confusion.
So when a patient is told, “You have nasal polyps,” the next question should be:
What kind of disease produced the polyp?
Without that answer, the term does not tell the patient enough.
Why “with polyps” and “without polyps” is no longer enough
For many years, chronic rhinosinusitis was divided into two broad groups:
- chronic rhinosinusitis with nasal polyps
- chronic rhinosinusitis without nasal polyps
This was simple, but it was too blunt.
It is similar to saying a patient has “chronic bronchitis with wheeze” or “chronic bronchitis without wheeze.” A wheeze is an examination finding. It may be widespread throughout the lungs, localised to one area, caused by asthma, caused by airway obstruction, or caused by something else entirely. The wheeze matters, but it does not define the disease.
The same applies to nasal polyps. The presence of polypoid tissue tells us something has happened to the mucosa. It does not, by itself, define the mechanism.
A polyp is a tissue remodelling event. The important question is why the tissue remodelled.
This is the same broader problem discussed in “septal deviation and big turbinates” is not a diagnosis . An examination finding is not the same as a disease mechanism.
The confusing world of “CRS with nasal polyps”
The problem is that the label CRS with nasal polyps collects many different processes under one heading.
A patient with eosinophilic diffuse type 2 CRS, a patient with allergic fungal rhinosinusitis, a patient with aspirin-exacerbated respiratory disease, a patient with cystic fibrosis, and a patient with a localised antrochoanal polyp may all be described as having “polyps.” But these are not the same disease.
This is why the old terminology can mislead patients, trainees and non-ENT clinicians. It describes what was seen, but not why it formed.
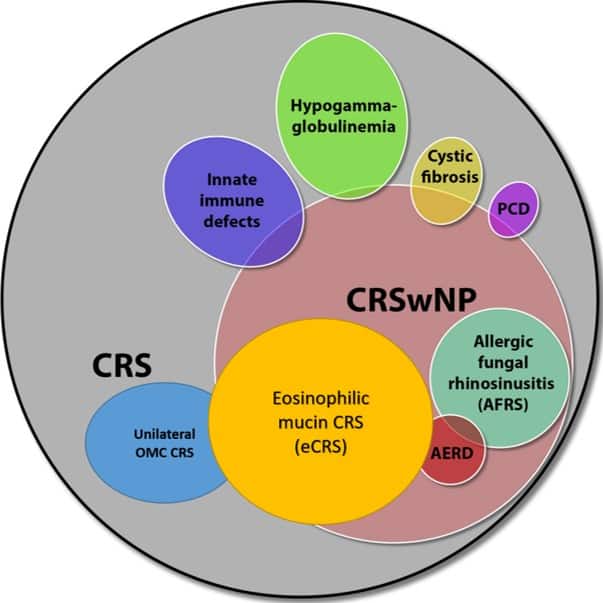
The confusing disease entities that are placed in the traditional CRS with and without polyps nomenclature. Adapted from Cho SH, Hamilos DL, Han DH, Laidlaw TM. Phenotypes of Chronic Rhinosinusitis. The Journal of Allergy and Clinical Immunology: In Practice. 2020;8(5):1505-11.
Caption: The term “CRS with nasal polyps” groups together multiple disease processes, including eosinophilic mucin CRS, allergic fungal rhinosinusitis, AERD, cystic fibrosis, immune defects and localised disease. The shared feature is polypoid tissue, not a single disease mechanism.
The word polyp is doing too much work.
EPOS 2020 tried to move the field forward
The European Position Paper on Rhinosinusitis and Nasal Polyps 2020, known as EPOS 2020, attempted to move the profession beyond the old “polyps versus no polyps” model.[1] EPOS 2020 proposed a more useful classification of chronic rhinosinusitis based on whether the disease is primary or secondary, whether it is localised or diffuse, and whether there is type 2 inflammatory dominance.
This matters clinically.
Primary CRS refers to inflammatory disease that is essentially limited to the respiratory airway. Secondary CRS occurs when sinus disease is part of another defined process, such as immunodeficiency, cystic fibrosis, granulomatosis with polyangiitis, odontogenic infection, or tumour.[1,2]
Primary CRS can then be considered by anatomical distribution:
- Localised CRS, usually affecting a discrete sinus region or functional drainage pathway
- Diffuse CRS, involving a broader inflammatory airway process
Diffuse does not necessarily mean every sinus is completely opaque on a CT scan. It means the disease is not confined to one simple anatomical unit. It is a broader airway inflammatory process.[1,2]
This framework is much more useful than simply saying “polyps are present.”
For a more detailed explanation of the EPOS 2020 classification system, this video discusses how CRS can be reorganised away from the older “polyps/no polyps” framework and toward primary versus secondary disease, localised versus diffuse disease, and type 2 versus non-type 2 inflammatory dominance.
CRS classification beyond polyps and no polyps
The same concept is discussed in more detail in the 2021 BJ Ferguson Lecture, “CRS: Moving beyond polyps/no polyps and the concepts of maximal medical therapy.” This lecture reviews how the EPOS 2020 working group reorganised CRS classification around phenotype and endotype, and how that framework places surgery, antibiotics, anti-inflammatory therapy and biologics into a more logical treatment strategy.
2021 BJ Ferguson Lecture: CRS classification beyond polyps/no polyps and the role of phenotype/endotype in treatment selection.
Different polyps mean different diseases
The confusion becomes clearer when we look at examples.
1. Classic diffuse type 2 CRS with polyps
This is what many clinicians historically meant by “nasal polyposis.” Patients develop significant bilateral polypoid inflammatory tissue, often associated with smell loss, asthma, aspirin-exacerbated respiratory disease, eosinophilic inflammation and recurrence after surgery.
In this setting, the polyp burden may become large enough to physically block topical medications from reaching the sinus cavities. Surgery may be needed to remove obstructing tissue and improve access for ongoing medical therapy. But surgery does not switch off the underlying inflammatory disease.
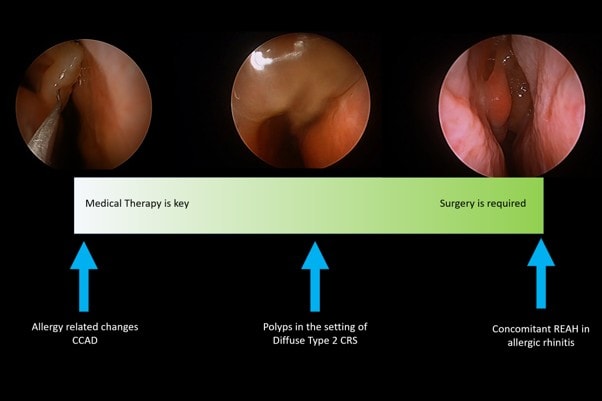
2. Central compartment atopic disease
Central compartment atopic disease, or CCAD, is different. Here, polypoid or oedematous change is concentrated in the central part of the nose, particularly around the middle turbinate, superior turbinate, superior septum and olfactory cleft region. It is commonly associated with inhalant allergy.[3]
These changes may look “polypoid,” but the treatment strategy is not the same as for advanced diffuse type 2 CRS. In many patients, the key is allergy-directed medical therapy, particularly allergen immunotherapy when persistent house dust mite or other inhalant allergy is driving chronic disease.
This links directly to the broader argument in Why Immunotherapy Should Not Be the Last Step in Allergic Rhinitis .
If the polypoid change is mainly a marker of allergic tissue remodelling, removing tissue without addressing the allergic driver is not a long-term strategy.
3. Respiratory epithelial adenomatoid hamartoma
Respiratory epithelial adenomatoid hamartoma, or REAH, is another example. It may appear as polypoid tissue, often in the olfactory cleft. But it is not simply inflammatory nasal polyposis. REAH is a benign glandular proliferation and is classified as a benign epithelial lesion of the sinonasal tract.[4]
This distinction matters because olfactory cleft tissue should not automatically be treated as a “no-go zone.” When the lesion is proliferative rather than just inflammatory swelling, early surgical removal may be appropriate.
4. Antrochoanal polyps
An antrochoanal polyp is usually an isolated lesion arising from the maxillary sinus and extending through the choana. It is a polyp, but it is not the same disease as diffuse type 2 CRS. It is usually treated surgically because it is a localised anatomical lesion.
5. Cystic fibrosis and other secondary causes
Patients with cystic fibrosis can develop nasal polyps. But this is not the same biological disease as adult eosinophilic diffuse type 2 CRS. Cystic fibrosis is a genetic disorder with different mucus, infection and epithelial transport mechanisms.
This is why a generic label such as “CRS with nasal polyps” is inadequate. A patient with cystic fibrosis and polyps should not be conceptually grouped with an adult with type 2 eosinophilic CRS simply because both have polypoid tissue in the nose.
The polyp is the shared appearance. The disease is different.
Treatment depends on the disease that made the polyp
This is the key clinical point.
Some polypoid changes are mainly a marker of allergic inflammation. In those patients, medical therapy is the centre of treatment. This may include topical corticosteroids, saline irrigation, allergen avoidance and allergen immunotherapy when inhalant allergy is driving chronic disease.
Some polyps are part of diffuse type 2 CRS. Medical therapy remains important, but established tissue remodelling can become too bulky, obstructive or anatomically fixed to resolve adequately with medication alone. Surgery may be needed to remove established inflammatory tissue, open the sinuses and allow topical therapy to reach the mucosa.
Some polypoid lesions, such as REAH in the olfactory cleft, are proliferative lesions. These should not be managed as if they were simply oedema from allergy.
Very different treatment focus – so confusing to trainees. I often get asked: “If I see polyps do i take them out?” but the polyp is the marker of an underlying condition.
Polypoid tissue can reflect different mechanisms. Allergy-related central compartment disease is primarily medically managed, diffuse type 2 CRS often requires combined medical and surgical care, and proliferative lesions such as REAH usually require surgery.
Why surgery is still needed when tissue remodelling is established
The idea that all nasal polyps should simply “melt away” with medication is not realistic.
Nasal polyps are a visible form of tissue remodelling. In CRS, remodelling can include epithelial damage, basement membrane thickening, fibrosis, squamous metaplasia, oedema and hyperplastic change.[5,6] In one study of 259 CRS patients, remodelling changes were present in 85% overall, and were more common in both CRSwNP and eosinophilic CRS.[5] Eosinophilic CRS was also associated with mucosal damage, including ulceration, oedema and hyperplastic change.[5]
This matters because tissue remodelling is not just “swelling.” It can represent structural change in the mucosa and submucosa. A later review of sinonasal tissue remodelling emphasised that remodelling may occur early and in parallel with inflammation, and that established CRS can require surgery to remove purulent, stagnant mucus and inflamed tissue when disease remains unresolved.[6]
The biology of polyp formation also supports this. Type 2 inflammation can drive plasma leakage, oedema and fibrin deposition. Takabayashi and Schleimer describe nasal polyp formation as involving type 2 inflammation, altered coagulation and reduced fibrinolysis, producing a fibrin-rich tissue environment.[7]
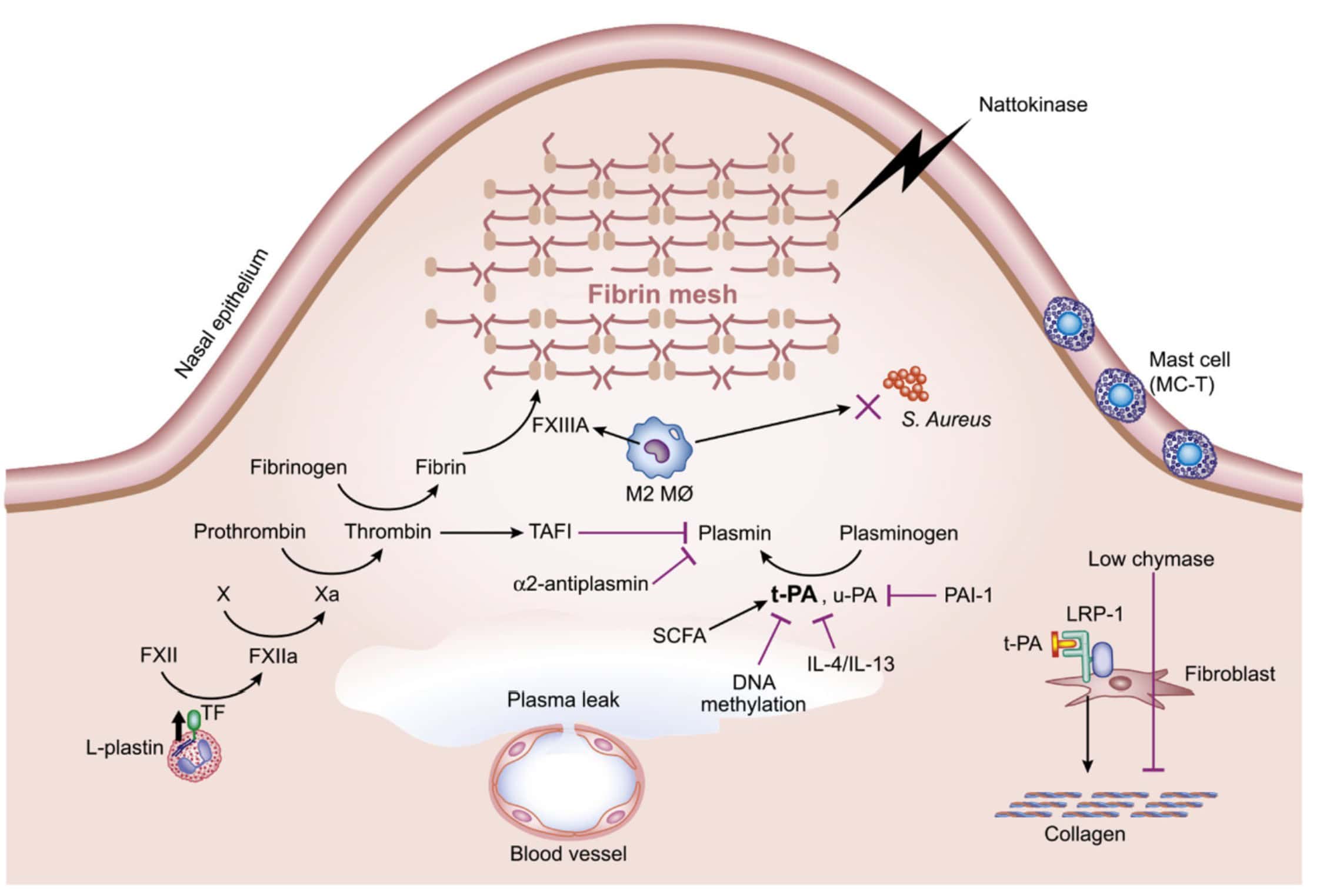
Takabayashi T, Schleimer RP. Formation of nasal polyps: The roles of innate type 2 inflammation and deposition of fibrin. J Allergy Clin Immunol 2020; 145:740-750.
Type 2 inflammation can promote plasma leakage, fibrin deposition, impaired fibrinolysis and stromal change. This helps explain why established nasal polyps are not simply transient mucosal swelling.
This is why surgery and medical therapy should not be viewed as opposing treatments. Surgery deals with established anatomy and obstructing remodelling. Medical therapy deals with the inflammatory mechanism that caused the remodelling.
In modern CRS care, remission usually requires both: control of the underlying inflammatory disease and removal of obstructive or irreversible tissue changes when they prevent effective ongoing treatment. This same principle is discussed in relation to remission and long-term CRS control in related rhinology research publications
Biologics have reinforced the old terminology
Unfortunately, just as rhinology was trying to move beyond “with polyps” and “without polyps,” biologic therapies entered the field using the older terminology.
In the United States, FDA-approved biologic indications have generally been framed around chronic rhinosinusitis with nasal polyps, or CRSwNP. Dupilumab, omalizumab, mepolizumab and tezepelumab all use this general disease label in their regulatory indication language.[8–11] Tezepelumab, for example, was approved in the United States in 2025 as add-on maintenance treatment for inadequately controlled CRSwNP in patients aged 12 years and older.[11]
Australia has followed similar terminology. The Therapeutic Goods Administration uses “chronic rhinosinusitis with nasal polyposis” or “chronic rhinosinusitis with nasal polyps” terminology in biologic indications and regulatory documents. Dupilumab and mepolizumab have Australian CRSwNP indications, and Tezspire has been listed by the TGA as under evaluation for a proposed CRSwNP indication.[12–14]
This regulatory terminology is understandable. Pharmaceutical approvals require a defined disease indication. The problem is that “CRSwNP” is still a very broad container. It does not adequately describe the underlying disease mechanism.
That creates ambiguity in clinical practice. Biologics can be very effective in selected patients with type 2 inflammatory CRS. But treatment responses vary. Some patients respond dramatically. Others respond partially. Some do not respond in a way that justifies long-term treatment cost or exposure.
Part of that variability reflects the fact that “CRSwNP” is not one disease.
Biomarkers help, but they do not solve the terminology problem
There have been attempts to use biomarkers to select patients for biologics. Blood eosinophils, serum IgE, tissue eosinophilia, asthma status, aspirin-exacerbated respiratory disease and smell loss can all help build a picture of type 2 inflammatory disease. EPOS 2020, for example, included evidence of type 2 inflammation, systemic corticosteroid need, impaired quality of life, smell loss and comorbid asthma in its criteria for considering biologic treatment in CRSwNP.[1]
But biomarkers do not fully solve the problem created by a weak disease label.
A raised eosinophil count may support type 2 inflammation, but it does not by itself define the anatomy, severity, comorbid disease, surgical state, infection burden or tissue remodelling pattern. A normal eosinophil count does not exclude local type 2 inflammation in the nose. A patient with polypoid tissue from another mechanism should not be expected to respond to a type 2 biologic just because the word “polyp” appears in the diagnosis.
This is why classification matters. Treatment should follow the mechanism, not just the appearance.
Radiology makes the problem worse
Patients are often told they have “polyps” after a CT scan. Sometimes the report is describing true polypoid inflammatory disease. Sometimes it is describing mucosal thickening. Sometimes it is describing a mucous retention cyst. Sometimes it is an incidental rounded area of mucosa within a sinus cavity.
A radiology report that says “polyps are seen in the sinuses” can cause unnecessary anxiety. It may also create the impression that there is a tumour-like growth that needs to be removed. In many cases, that is not true.
A nasal endoscopy and clinical context are usually needed to interpret what the finding means. Symptoms such as blockage should also be interpreted carefully, because nasal congestion is not always the same as nasal obstruction and imaging findings alone do not always explain the patient’s experience.
This also overlaps with the concept of functional nasal obstruction , where symptoms and visible structural findings may not align neatly.
What patients should ask
If a patient is told they have nasal polyps, the useful questions are:
- Are these inflammatory polyps or another type of lesion?
- Are they localised or diffuse?
- Is this primary airway disease or secondary to another condition?
- Is simple inhalant allergy driving the changes?
- Is surgery needed to remove obstructing tissue, or is medical therapy the main treatment, or is a combination of both required?
- If biologics are being considered, what disease mechanism are they targeting?
When symptoms are persistent or confusing, assessment may require more than simply looking at a CT scan. Objective nasal airflow and allergy testing can help clarify whether the main problem is mucosal inflammation, allergy, airflow limitation, structural obstruction or a mismatch between symptoms and anatomy.
These questions move the conversation from “there is a polyp” to “what disease process is present?”
What clinicians should say instead
Rather than saying:
“You have nasal polyps.”
A better explanation is:
“You have polypoid tissue in the nose. That tells us the lining has remodelled, but we need to work out why. The treatment depends on the disease that produced the polyp.”
That single sentence changes the discussion. It separates the finding from the diagnosis.
Conclusion
A nasal polyp is not a disease. It is a visible result of tissue change.
The old classification of chronic rhinosinusitis with or without nasal polyps is no longer fit for purpose. It is too broad for patients, too imprecise for trainees, and too weak for modern treatment decisions involving surgery, immunotherapy and biologics.
EPOS 2020 and contemporary CRS classification have tried to move the field toward a better framework: primary versus secondary disease, localised versus diffuse anatomy, and type 2 versus non-type 2 inflammatory dominance.[1,2]
That is the right direction.
Some polypoid changes are markers of allergy and need medical therapy. Some are obstructive inflammatory tissue requiring surgery as part of disease control. Some are benign proliferative lesions that should be removed. Some occur in systemic or genetic diseases where the mechanism is completely different.
The word “polyp” is therefore only the start of the conversation.
The real diagnosis comes from understanding the disease that made it.
References
- Fokkens WJ, Lund VJ, Hopkins C, Hellings PW, Kern R, Reitsma S, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1–464.
- Grayson JW, Hopkins C, Mori E, Senior B, Harvey RJ. Contemporary classification of chronic rhinosinusitis beyond polyps vs no polyps: a review. JAMA Otolaryngol Head Neck Surg. 2020;146(9):831–838. doi:10.1001/jamaoto.2020.1453.
- DelGaudio JM, Loftus PA, Hamizan AW, Harvey RJ, Wise SK. Central compartment atopic disease. Am J Rhinol Allergy. 2017;31(4):228–234.
- Thompson LDR, Franchi A. New tumor entities in the 4th edition of the World Health Organization classification of head and neck tumors: nasal cavity, paranasal sinuses and skull base. Virchows Arch. 2018;472(3):315–330.
- Barham HP, Osborn JL, Snidvongs K, Mrad N, Sacks R, Harvey RJ. Remodeling changes of the upper airway with chronic rhinosinusitis. Int Forum Allergy Rhinol. 2015;5(7):565–572. doi:10.1002/alr.21546.
- Amirapu S, Biswas K, Radcliff FJ, Mackenzie BW, Ball S, Douglas RG. Sinonasal tissue remodelling during chronic rhinosinusitis. Int J Otolaryngol. 2021;2021:7428955. doi:10.1155/2021/7428955.
- Takabayashi T, Schleimer RP. Formation of nasal polyps: the roles of innate type 2 inflammation and deposition of fibrin. J Allergy Clin Immunol. 2020;145(3):740–750. doi:10.1016/j.jaci.2020.01.027.
- U.S. Food and Drug Administration. DUPIXENT (dupilumab) injection, for subcutaneous use: prescribing information.
- U.S. Food and Drug Administration. XOLAIR (omalizumab) injection, for subcutaneous use: prescribing information.
- U.S. Food and Drug Administration. NUCALA (mepolizumab) injection, for subcutaneous use: prescribing information.
- U.S. Food and Drug Administration. TEZSPIRE (tezepelumab-ekko) injection, for subcutaneous use: prescribing information.
- Therapeutic Goods Administration. DUPIXENT (dupilumab): chronic rhinosinusitis with nasal polyposis indication.
- Therapeutic Goods Administration. NUCALA (mepolizumab): chronic rhinosinusitis with nasal polyps indication.
- Therapeutic Goods Administration. TEZSPIRE (tezepelumab): prescription medicine under evaluation for chronic rhinosinusitis with nasal polyps.
Frequently Asked Questions
Is a nasal polyp a diagnosis?
No. A nasal polyp is usually an examination finding. It describes polypoid tissue in the nose, but it does not explain why that tissue formed. Different diseases can produce nasal polyps, so the underlying mechanism matters.
What causes nasal polyps?
Nasal polyps can form through several mechanisms. Some are related to diffuse type 2 inflammation in chronic rhinosinusitis. Others are associated with inhalant allergy, aspirin-exacerbated respiratory disease, allergic fungal rhinosinusitis, cystic fibrosis, localised lesions such as antrochoanal polyps, or benign proliferative lesions such as respiratory epithelial adenomatoid hamartoma.
Why is the term “chronic rhinosinusitis with nasal polyps” confusing?
The term groups many different disease processes under one label. It tells us that polypoid tissue is present, but it does not define whether the disease is localised or diffuse, primary or secondary, type 2 or non-type 2, allergic, genetic, infectious, inflammatory or proliferative.
What did EPOS 2020 change about CRS classification?
EPOS 2020 moved chronic rhinosinusitis classification toward primary versus secondary disease, localised versus diffuse disease, and type 2 versus non-type 2 inflammatory dominance. This is more useful than simply dividing CRS into “with polyps” and “without polyps.”
Do all nasal polyps need surgery?
No. Some polypoid changes are mainly markers of allergic inflammation and may be managed medically. Other polyps become obstructive or anatomically fixed and require surgery to remove established tissue remodelling. Some proliferative lesions, such as REAH, are usually treated surgically.
Why might surgery still be needed if biologics are available?
Biologics can reduce type 2 inflammation in selected patients, but established polypoid tissue may represent structural remodelling rather than simple swelling. Surgery may still be needed to remove obstructive tissue, open the sinuses and allow topical medical therapy to reach the diseased mucosa.
Are biologics suitable for all patients with nasal polyps?
No. Biologics are most relevant when the underlying mechanism is type 2 inflammatory disease. A patient with polyps from a different mechanism, such as cystic fibrosis or a localised proliferative lesion, should not be expected to respond in the same way simply because the word “polyp” appears in the diagnosis.
What should patients ask if they are told they have nasal polyps?
Patients should ask what kind of disease produced the polyp. Useful questions include whether the polyps are inflammatory or another lesion, whether disease is localised or diffuse, whether it is primary airway disease or secondary to another condition, whether inhalant allergy is driving the changes, and whether treatment should be medical, surgical or both.